 CN
CN
Ceftazidime for Injection
Instructions for Ceftazidime for Injection
Please read the instructions carefully and a physician or pharmacist use under the guidance of
[Name of the drug]
Generic name: Ceftazidime for Injection
Product name: Ceftazidime for Injection
Hanyu Pinyin: Zhusheyong Toubaotading
[Ingredients]
The active ingredient in this product is ceftazidime.
Chemical Name: (6 R R,7 R )-7-[[(2-amino-4-thiazolyl)-[(L-carboxy-1-methylethoxy)imino]acetyl]amino]-2-carboxy-8-oxo-5-thio-1-azabiabicyclic
[4.2.0]oct-2-en-3-methylpyridium intrasalt pentahydrate
Chemical structural formula:
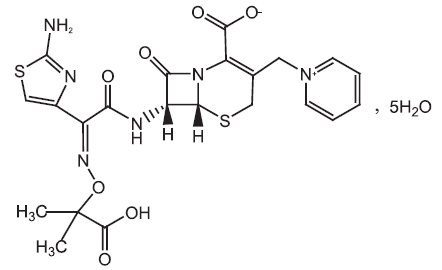
Molecular formula: C 22 H 22 N 6 O 7 S 2 ·5H 2 O
Molecular weight: 636.65
Excipients: anhydrous sodium carbonate
[Characteristics]
This product is a white or white-like crystalline powder.
[Indications]
This product is suitable for the treatment of single or multiple infections caused by sensitive microorganisms.
1. Systemic severe infections: Systemic severe infections caused by Pseudomonas spp. (including
Pseudomonas aeruginosa), Haemophilus influenzae (including
ampicillin-resistant strains), Klebsiella spp. (including Klebsiella
pneumoniae), Enterobacteriaceae spp., Proteus spp., Escherichia coli,
Serratia spp., Citrate spp., Streptococcus pneumoniae, and
Staphylococcus aureus (methicillin-sensitive strains), such as: sepsis,
bacteremia, peritonitis, Infections in immunosuppressed patients and
infections in intensive care patients (eg, burn infections).
2. Lower respiratory tract infections (including pneumonia): caused by Pseudomonas spp. (including Pseudomonas aeruginosa),
Haemophilus influenzae (including ampicillin-resistant strains),
Klebsiella spp. (including Klebsiella pneumoniae), Enterobacteriaceae
spp., Proteus mira, Escherichia coli, Serratia spp., Citrate spp.,
Streptococcus pneumoniae, and Staphylococcus aureus
(methicillin-sensitive strains).
3. ENT infections: caused by Pseudomonas spp. (including Pseudomonas aeruginosa),
Haemophilus influenzae (including ampicillin-resistant strains),
Streptococcus pneumoniae, Staphylococcus aureus (methicillin-sensitive
strains), and Streptococcus pyogenes (group A β hemolytic
streptococcus).
4. Urinary tract infections: caused by Pseudomonas spp. (including Pseudomonas aeruginosa),
Enterobacteriaceae, Proteus spp. (including Proteus mirables and
indole-positive Proteus), Klebsiella spp. and Escherichia coli.
5. Skin and soft tissue infections: caused by Pseudomonas aeruginosa, Klebsiella spp., Escherichia coli,
Proteus spp. (including Proteus mirables and Indole-positive Proteus),
Enterobacteriaceae, Serratia, Staphylococcus aureus
(methicillin-sensitive strains), and Streptococcus pyogenes (group A β
hemolytic streptococcus).
6. Bone and joint infections: caused by Pseudomonas aeruginosa, Klebsiella spp., Enterobacteriaceae
spp., and Staphylococcus aureus (methicillin-sensitive strains).
7. Gynecological infections: including endometritis, pelvic cellulitis, and other female genital tract infections caused by Escherichia coli.
8. Gastrointestinal, biliary and abdominal infections: including peritonitis caused by Escherichia coli, Klebsiella spp. and
Staphylococcus aureus (methicillin-sensitive strains), as well as
multiple microbial infections caused by aerobic and anaerobic
microorganisms and Bacteroidetes (note: many Bacteroides fragilis
strains are resistant).
9. Hematological/peritoneal dialysis and persistent ambulatory peritoneal dialysis (CAPD)-related infections: caused by Pseudomonas aeruginosa, Escherichia coli, Enterobacteriaceae
spp., and Staphylococcus aureus (methicillin-sensitive strains).
10. Central nervous system infections (including meningitis): caused by Haemophilus influenzae and Neisseria meningitidis. In
addition, ceftazidime has been successfully used in several cases of
meningitis caused by Pseudomonas aeruginosa and Streptococcus
pneumoniae.
11. Prevention of perioperative urinary tract infections: for patients undergoing prostate surgery (transurethral resection).
May be used alone in patients with meningitis confirmed by sensitive test results.
It can be used in infections resistant to other antimicrobials, including aminoglycosides and cephalosporins.
It can be used in combination with aminoglycosides or most other β-lactam antibiotics.
When Bacteroides fragilis infection is suspected, it may be combined with another anti-anaerobic antibacterial drug.
Sensitivity to ceftazidime varies by region and time, and local
susceptibility data should be consulted as appropriate (see Pharmacology
and Toxicology).
[Specifications]
As C 10 p.m. :22 N 6 O 7 S 2 计 (1)0.75g (2)1.5g
[Usage and dosage]
Ceftazidime is given parenterally, and the dose depends on the severity
of the infection, susceptibility, type of infection, and the patient's
age, weight, and kidney function.
Adults:
The adult dose range for ceftazidime is 1 g to 6 g per day, given
intravenously or intramuscularly every 8 hours or every 12 hours. For
most infections, a dose of 1 g every 8 hours or 2 g every 12 hours
should be given, and for urinary tract infections and many milder
infections, 500 mg or 1 g per 12 hours is generally sufficient. For
severe gynecological and intra-abdominal infections, an intravenous dose
of 2 g every 8 hours should be given. For very serious infections,
especially immunosuppressed patients, including those with neutropenia, a
dose of 2 g every 8 or 12 hours or a dose of 3 g every 12 hours should
be given.
When used as prophylaxis for prostate surgery, a dose of 1 g should be
used during induction of anesthesia, and a second dose should be
considered for catheter removal.
Elderly patients:
In view of the reduced clearance of ceftazidime in the acutely ill
elderly, especially in patients older than 80 years, the daily dose
should generally not exceed 3 g.
Cystic fibrosis:
For adult patients with fibrocystic lung infection with normal renal
function and Pseudomonas, a high dose of 100~150mg/kg per day according
to body weight should be used in three doses. For adults with normal
kidney function, the dose can reach 9g per day.
Infants and children:
For children over 2 months of age, the general dose range is 30~100mg/kg
per day according to body weight, given in two or three doses.
For children with infection who are immunosuppressed or have fibrotic
cysts, or children with meningitis, doses as high as 150 mg/kg per day
(maximum dose of 6 g per day) can be given in three doses.
Newborn to 2 months of age infants:
Clinical experience is limited, and the general dose is 25~60mg/kg per
day according to body weight, which has been proven to be effective in
two doses. Newborn infants have a ceftazidime serum half-life three to
four times that of adults.
Dosage in case of renal impairment:
Ceftazidime is almost entirely excreted from the kidneys through
glomerular filtration. Therefore, the dose should be reduced in patients
with renal impairment to compensate for the slowed excretory function,
except in patients with mild renal impairment (i.e., glomerular
filtration rate (GFR) greater than 50 ml/min). For patients with
suspected renal insufficiency, a first loading dose of 1 g may be given,
and then the appropriate maintenance dose should be determined based on
the glomerular filtration rate.
For patients with renal failure who are receiving continuous
arteriovenous or high-throughput hemodialysis in the intensive care
unit, the recommended dose is 1 g per day in divided doses. For patients
on low-throughput hemodialysis, the recommended dose for renal
insufficiency should be referenced.
The recommended maintenance dose is as follows:
In renal insufficiency, the recommended maintenance dose of ceftazidime
| Creatinine clearance (ml/min). | Serum creatinine is approximately μmol/L (mg/dl). | Ceftazidime single dose (g). | Frequency of administration (once an hour). |
| 50-31 | 150-200 (1.7-2.3) |
1 | 12 |
| 30-16 | 200-350 (2.3-4.0) |
1 | 24 |
| 15-6 | 350-500 (4.0-5.6) |
0.5 | 24 |
| <5 | >500 (>5.6) |
0.5 | 48 |
*The values listed above do
not accurately predict kidney function in all patients, especially in
older patients whose serum creatinine clearance may be too high to
assess kidney function.
For patients with severe infection, especially those with neutropenia, a
dose of 6g of ceftazidime per day is generally received, but it cannot
be used for patients with renal insufficiency. The single dose listed in
the table above can be increased by 50% or the frequency of
administration may be increased appropriately. For these patients, it is
recommended to monitor serum concentrations of ceftazidime, and trough
concentrations should not exceed 40 mg/L.
When only serum creatinine concentrations are available, the following
formula (Cockcroft formula) is used to estimate creatinine clearance.
Serum creatinine clearance represents a steady state of renal function:
Male:
Creatinine clearance = body weight (kg) × (140-age).
(ml/min) 72× serum creatinine concentration (mg/dl).
Female:
0.85× or more
Serum creatinine is divided by 88.4, which can be converted from μmol/L to mg/dl.
Creatinine clearance in children should be adjusted for body surface
area or fat-free weight. For children with renal insufficiency, the
frequency of dosing should be reduced as in adults.
During hemodialysis, ceftazidime has a serum half-life of 3 to 5 hours.
After each hemodialysis, the appropriate maintenance dose of ceftazidime
should be repeated.
Dosage of peritoneal dialysis:
Ceftazidime can be used for peritoneal dialysis and continuous
peritoneal dialysis (CAPD). Like intravenous ceftazidime, it can be
added to dialysis fluid (usually 125 mg or 250 mg in 2 liters of
dialysis solution).
Method of administration
Ceftazidime can be given intravenously or by deep intramuscular
injection, such as the lateral quarter above the gluteus maximus or the
lateral part of the thigh.
Modulation Instructions: The amount of dilution and solution
concentration are shown in the table below, which may be useful when
partial dose is required.
Modulation of the solution:
| Bottle quantity | The amount of dilution (ml) needs to be added | Approximate concentration (mg/ml). |
| 250mg intramuscularly | 1.0 | 210 |
| 250mg intravenously | 2.5 | 90 |
| 500mg intramuscularly | 1.5 | 260 |
| 500mg intravenously | 5.0 | 90 |
| 1g intramuscularly | 3.0 | 260 |
| 1g IV | 10.0 | 90 |
| 2g intravenous bolus | 10.0 | 170 |
| 2g IV drip | 50.0* | 40# |
| 3g intravenous bolus | 15.0 | 170 |
| 3g intravenous drip | 75.0* | 40# |
Note:
*The addition of the solution should be divided into two steps.
#使用0.9% sodium chloride injection, 5% glucose injection, or other
approved dilutions (see Notes) because water for injection produces a
hypotonic solution at this concentration.
All bottles of ceftazidime injections are decompression. When the drug
dissolves, it releases carbon dioxide, which creates positive pressure.
For ease of use, the following modulation techniques are recommended:
250mg intramuscular or intravenous, 500mg intramuscular or intravenous,
1g intramuscular or intravenous, 2g or 3g intravenous bolus:
1. Insert the syringe needle into the seal of the medicine bottle,
inject the recommended dose of dilution, and pull out the needle.
2. Shake until dissolved, release carbon dioxide, and form a clear solution after 1-2 minutes.
3. Turn the bottle upside down, push the syringe core to the head,
insert the needle into the medicine bottle seal, and all the solution
will be sucked into the syringe (the pressure in the bottle will promote
the solution to be inhaled), keeping the needle in the solution. The
tiny bubbles of carbon dioxide in the solution can be ignored.
These solutions can be injected directly into a vein or directly into a
tube where the drug is administered when the patient receives parenteral
fluids. Ceftazidime may be compatible with commonly used intravenous
solutions.
The bottled injection does not contain any preservatives and is therefore intended for use as a single dose only.
To comply with the management requirements of the preparation, it is
best to use newly formulated ceftazidime injection. If this is not
possible, store it in the refrigerator at 2~8°C for 24 hours to maintain
the effect.
(When the dilution is water for injection or any of the injections listed below).
In the following solutions, the concentration of ceftazidime is 1~40mg/ml:
0.9% sodium chloride injection;
M/6 Sodium Lactate Injection;
compound sodium lactate injection (Hartmann's solution);
5% glucose injection;
0.225% sodium chloride and 5% glucose injection;
0.45% sodium chloride and 5% glucose injection;
0.9% sodium chloride and 5% glucose injection;
0.18% sodium chloride and 4% glucose injection;
10% glucose injection;
10% of dextran 40 injection in 0.9% sodium chloride injection;
10% of dextran 40 injection in 5% glucose injection;
6% of dextran 70 injection in 0.9% sodium chloride injection;
6% of dextran 70 injection in 5% glucose injection;
(Ceftazidime is less stable than other intravenous fluids in sodium
bicarbonate injection, so it is not recommended to use this injection as
a dilution.) )
The concentration of ceftazidime in peritoneal dialysis solution (lactate) is 0.05mg~0.25mg/ml.
Ceftazidime for intramuscular injection can be prepared with 0.5% or 1% lidocaine hydrochloride injection.
When the concentration of ceftazidime is 4mg/ml, it is mixed with the following drugs, and both maintain good efficacy:
Hydrocortisone (hydrocortisone sodium phosphate) 1mg/ml in 0.9% sodium chloride injection or 5% glucose injection;
Cefuroxime (cefuroxime sodium) 3mg/ml in 0.9% sodium chloride injection;
o-chlorpenicillin (o-chlorpenicillin sodium) 4mg/ml in 0.9% sodium chloride injection;
Heparin 10IU/ml or 50 IU/ml in 0.9% sodium chloride injection;
Potassium chloride 10 mEq/L or 40 mEq/L in 0.9% sodium chloride injection.
The color of the formulated injection ranges from light yellow to amber,
depending on the concentration, dilution and storage conditions, and
the efficacy of the product will not be affected by color differences
when used according to the recommendation.
[Adverse reaction]
Data to determine the types of adverse effects that occur with frequency
ranging from very common to uncommon are obtained from large-scale
clinical studies, both internal and published. For the frequency of
other adverse effects, post-market surveillance data is used primarily
and is usually based on reporting rates rather than actual frequency.
The classification of the frequency of adverse reactions is defined as:
Very common≥ 1/10
Common ≥ 1/100 and < 1/10
Uncommon≥ 1/1000 and < 1/100
Rare ≥ 1/10000 and < 1/1000
Very rare< 1/10000
Infections and invasive diseases
Uncommon: Candidiasis (including vaginitis and oral thrush).
Disorders of the blood and lymphatic system
Common: eosinophilia and thrombocytosis
Uncommon: leukopenia, neutropenia, and thrombocytopenia
Very rare: lymphocytosis, hemolytic anemia and agranulocytosis
Immune system disorders
Very rare: allergic reactions (including bronchospasm or low blood pressure).
Nervous system disorders
Uncommon: headache, dizziness
Very rare: paresthesia on the skin
Neurological sequelae have been reported when this product is not
properly reduced in patients with kidney damage, including: tremors,
myoclonus, convulsions, encephalopathy, and coma.
Disorders of the vascular system
Common: Phlebitis or thrombophlebitis due to intravenous administration
Gastrointestinal disorders
Common: Diarrhea
Uncommon: nausea, vomiting, abdominal pain, and colitis
Very rare: poor taste
Like other cephalosporins, colitis may be associated with Clostridium
difficile and may present as pseudomembranous colitis (see Precautions).
Hepatobiliary disorders
Common: Transient elevations in one or more liver enzymes, including:
ALT (SGPT), AST (SOGT), lactate dehydrogenase (LDH), glutamyltransferase
(GGT), and alkaline phosphatase.
Very rare: jaundice
Disorders of the skin and subcutaneous tissue
Common: maculopapular rash or urticaria
Uncommon: pruritus
Very rare: angioedema, erythema multiforme, Stevens-Johnson syndrome, and toxic epidermal necrolysis have been reported.
Systemic disorders and injection site reactions
Common: Pain and/or inflammation at the injection site after intramuscular injection.
Uncommon: Fever
Laboratory tests
Common: Coombs' test positive
Uncommon: As with other cephalosporins, transient elevations in blood
urea, blood urea nitrogen, and/or serum creatinine are observed.
Only 5% of patients have a positive Coombs' test and may affect blood cross-matching.
[Contraindication]
Ceftazidime is contraindicated in patients who are allergic to cephalosporin antibiotics;
It is contraindicated for patients who are allergic to ceftazidime pentahydrate or any of the excipients of this injection.
[Precautions]
Warning:
1. Before using this product for treatment, the patient should be
carefully asked whether there is a history of allergy to ceftazidime,
cephalosporins, penicillin or other drugs. This product is used with
caution in the treatment of patients with penicillin allergy because
cross-allergic reactions between β-lactam antimicrobials have been
clearly reported, and the incidence is as high as 10% in patients with a
history of penicillin allergy. If an allergic reaction occurs with
ceftazidime, stop taking the drug. Severe acute anaphylaxis may require
epinephrine and other first aid measures as clinically indicated,
including oxygen, intravenous fluids, intravenous antihistamines,
corticosteroids, vasopressors, and maintaining airway patency.
2. Almost all antibacterial drugs (including this product) have been
reported with Clostridium difficile-associated diarrhea (CDAD), the
severity of which can be manifested from mild diarrhea to fatal colitis.
Antimicrobial therapy can cause changes in the normal flora in the
colon, leading to overgrowth of C. difficile.
Toxins A and B produced by Clostridium difficile are associated with the
pathogenesis of CDAD. Clostridium difficile, which produces hypertoxin,
can lead to increased morbidity and mortality, and these infections may
be difficult to treat with antimicrobials, so colectomy may be
necessary. The possibility of CDAD must be considered in all patients
with diarrhea after antibiotic use. Since CDAD has been reported after
more than 2 months of antimicrobial therapy, a careful medical history
is required.
If CDAD is suspected or confirmed, consider discontinuation of
antibiotics that are not against Clostridium difficile. Fluid,
electrolyte, and protein supplementation must be appropriately based on
clinical indications, and antibiotics effective against Clostridium
difficile must be given, and surgical evaluation must be performed if
necessary.
3. Elevated ceftazidime levels in patients with renal insufficiency may
cause seizures, nonconvulsive status epilepticus (NCSE) encephalopathy,
coma, flapping tremor, neuromuscular excitement, and myoclonus.
General Notes:
1. Renal function:
Patients who are receiving nephrotoxic drugs (e.g., aminoglycoside
antibiotics, or strong diuretics such as furaniline) should be cautioned
when using high-dose cephalosporin antibiotics. Because the combination
of these drugs will affect kidney function. Clinical experience with
ceftazidime has shown that these problems generally do not occur at the
recommended dose. There is no evidence that normal therapeutic doses of
ceftazidime affect kidney function.
In patients with transient or persistent decreased urine output due to
renal insufficiency, high plasma concentrations of ceftazidime may occur
with prolonged duration with conventional doses. For patients with
renal insufficiency, the total daily dose of ceftazidime should be
reduced (see Dosage). Elevated ceftazidime levels in these patients may
cause seizures, nonconvulsive status epilepticus (NCSE) encephalopathy,
coma, flapping tremor, neuromuscular excitement, and myoclonus.
Subsequent doses should be determined based on the degree of renal
impairment, the severity of the infection, and the susceptibility of the
pathogenic organism.
2. Overgrowth of non-sensitive bacteria:
As with other broad-spectrum antimicrobials, long-term use of
ceftazidime may cause overgrowth of non-sensitive bacteria (e.g.,
Candida spp., Enterococcus) and may require termination of treatment or
appropriate measures. The patient's condition must be judged repeatedly.
Pseudomembranous colitis has been reported with antimicrobial use,
ranging in severity from mild to life-threatening. Therefore, it is
important that the above diagnosis should be taken into account in
patients who have diarrhea during or after the use of antimicrobials. If
the patient has prolonged or severe diarrhea or unusual abdominal pain,
treatment should be stopped immediately and the patient should be
further examined.
3. Resistance of sensitive bacteria:
As with other broad-spectrum cephalosporins and penicillins, some
bacterial genera that are originally sensitive to this product, such as
Escherichia coli and Serratia, may develop resistance during the
treatment with this product. Therefore, susceptibility tests should be
conducted regularly during the treatment of infections of the above
bacterial genus.
There is a need for local information on the prevalence of
drug-resistant and ultra-broad-spectrum β-lactamase-producing
(ESBLs)-producing bacteria, especially in the treatment of severe
infections.
4. This product should be used with caution in patients with a history of gastrointestinal diseases (especially colitis).
5. Cephalosporins may be related to decreased prothrombin activity. This
risk exists in patients with hepatic and renal impairment,
malnutrition, and long-term antimicrobial therapy. Patients at this risk
should be monitored for prothrombin time and treated with exogenous
vitamin K if necessary.
6. If ceftazidime is accidentally injected into the artery, it will cause distal necrosis.
7. In the absence of a confirmed or highly suspected bacterial
infection, or no indications for prevention, the use of this product may
not be beneficial to the patient and will increase the risk of
drug-resistant bacteria.
8. Compatibility taboos:
The stability of ceftazidime in sodium bicarbonate injection is lower
than that of other intravenous injections, so it is not recommended to
use this injection as a dilution.
Ceftazidime should not be mixed with aminoglycoside antibiotics in the same delivery system or syringe.
Precipitation has been reported when vancomycin is added to the prepared
ceftazidime injection. Therefore, during the administration of the two
drugs, the delivery system and the intravenous system must be flushed
with caution.
Ceftazidime contains 52 mg of sodium per 1 g, which must be considered for patients who need to limit sodium intake.
9. The impact on driving and mechanical ability has not been reported.
[Medication for pregnant and lactating women]
There are no trials showing that ceftazidime causes embryonic
malformations or teratogenic effects. But like all medications, it
should be used with caution in the first trimester and the first few
months of pregnancy. In pregnant women, use should be weighed against
the expected benefits than possible dangers.
Low concentrations of ceftazidime can be excreted into milk through the
breast glands, and lactating women should be cautious when using
ceftazidime.
[Children's medication]
See [Usage and Dosage]
[Medication for the elderly]
A total of 2221 participants were treated with ceftazidime in 11
clinical studies, of which 824 (37%) were aged 65 years or older and 391
(18%) were 75 years or older. No overall differences in safety and
efficacy between these and younger subjects were observed, and other
reported clinical trials did not show differences between older and
younger participants, but it is not ruled out that some older
individuals have higher sensitivity to drugs. It is known that this
product is basically excreted through the kidneys, and patients with
kidney injury are at a higher risk of toxic reactions when using this
product.
Because older patients may have weakened renal function, the dose should
be carefully selected and renal function monitored (see [Dosage]).
[Drug Interactions]
Nephrotoxicity has been reported in combination with cephalosporins and
aminoglycoside antimicrobials or strong diuretics such as furosemide.
Due to the potential nephrotoxicity and ototoxicity of aminoglycoside
antimicrobials, renal function should be carefully monitored, especially
when high-dose aminoglycosides or extended therapy is applied.
Nephrotoxicity and ototoxicity with ceftazidime alone have not been
observed in clinical trials.
Like other antimicrobials, this product may affect the gut microbiota,
leading to decreased estrogen reabsorption and reduced efficacy of
concomitant oral contraceptives.
Ceftazidime does not interfere with enzymatic tests for the
determination of urine glucose, but may interfere slightly with copper
reduction methods (Benedict's test, Ferrin test, and urine glucose
reagent tablet test).
Ceftazidime does not interfere with the identification of alkaline
picric acid of creatinine. About 5% of patients showed a positive Coombs
test related to the use of ceftazidime, which may interfere with
cross-matching tests of blood.
In vitro, chloramphenicol has antagonistic effects with ceftazidime and
other cephalosporins, and its clinical relevance is not known, but the
possibility of antagonism should be considered when recommending the use
of ceftazidime and chloramphenicol together.
[Drug overdose]
Ceftazidime overdose occurs in patients with pre-existing renal failure,
with reactions including seizures, encephalopathy, flapping tremor,
neuromuscular excitement, and coma. Patients with acute drug overdose
should be carefully observed and given supportive care. In the case of
renal insufficiency, hemodialysis and peritoneal dialysis can help
reduce serum ceftazidime concentrations.
[ Clinical Pharmacology]
Pharmacokinetics
Ceftazidime reaches high serum concentrations when administered
parenterally and persists for a long time. After intramuscular injection
of 500 mg and 1 g, the average serum peak concentrations reached 18
mg/L and 37 mg/L, respectively. Intravenous bolus of 500 mg, 1 g or 2 g,
the average serum concentration reached 46 mg/L, 87 mg/L and 170 mg/L
after 5 minutes, respectively. Serum concentrations remain at effective
therapeutic levels after 8 to 12 hours of intravenous and intramuscular
administration. The serum half-life is approximately 1.8 hours for
healthy volunteers and 2.2 hours for patients with normal renal
function. Ceftazidime has a low binding rate to serum proteins, about
10%.
Ceftazidime is not metabolized in the body, but is excreted into the
urine through glomerular filtration as a prototype drug, and about 80%
to 90% of the dose can be found in the urine within 24 hours. Less than
1% is excreted through bile, which significantly limits the amount that
enters the intestines. In tissues, such as bone, heart, bile, sputum,
aqueous humor, synovial fluid, pleural fluid and peritoneal fluid, the
concentration of ceftazidime can reach the minimum inhibitory
concentration of common pathogenic bacteria. Ceftazidime easily crosses
the placenta. Ceftazidime has a poor ability to penetrate the intact
blood-brain barrier, so its concentration in the cerebrospinal fluid is
low when inflammation is not present. When the meninges are inflamed,
the therapeutic concentration in the cerebrospinal fluid reaches 4-20
mg/L or higher.
[Pharmacology and Toxicology]
Pharmacological effects
Mechanism of action
Ceftazidime produces bactericidal activity by inhibiting bacterial cell
wall synthesis. Ceftazidime remains antimicrobial active in the presence
of some β-lactamases, including penicillinase and cephalosporinase in
gram-negative and gram-positive bacteria.
Drug resistance mechanism
The resistance mechanisms of ceftazidime are mainly hydrolysis of
β-lactamase, changes in penicillin-binding proteins (PBPs), and
decreased membrane permeability.
Interactions with other antimicrobials
In vitro studies, ceftazidime was combined with chloramphenicol and antagonistic effects were observed.
Ceftazidime exhibits antimicrobial activity against the vast majority of
the following bacteria, including in vitro testing and clinical
infections described under [Indications].
Gram-negative bacteria
· Citrate bacillus
· Enterobacteriaceae
· Escherichia coli
· Klebsiella genus
· Haemophilus influenzae
· Neisseria meningitidida
· Proteus miraculous
· Proteus vulgaris
· Pseudomonas aeruginosa
· Serratia spp
Gram-positive bacteria
· Staphylococcus aureus
· Streptococcus pneumoniae
· Streptococcus pyogenes
· Streptococcus lactate
Anaerobic bacteria
Bacteroides (Note: many Bacteroidetes isolates are resistant).
The following in vitro trial data have been obtained, but their clinical
significance is unknown. In addition, at least 90% of the following
bacteria showed a minimum inhibitory concentration (MIC) in vitro less
than or equal to the ceftazidime sensitive breakpoint. However, the
clinical effectiveness of ceftazidime in the treatment of infections
caused by these genera has not been verified in adequate and
well-controlled clinical trials.
Gram-negative bacteria
· Acinetobacter spp
· Differential Citrate
· Citrate freundii
· Providence genus (including Providence reiferia).
· Salmonella
· Shigella spp
· Haemophilus parainfluenzae
· Morganella Morse
· Neisseria gonorrhea
· Yersinia enterocolitis
Gram-positive bacteria
· Staphylococcus epidermidis
Anaerobic bacteria
· Clostridium genus (excluding Clostridium difficile).
· Digestive Streptococcus
Sensitivity test method
Where possible, clinical microbiology laboratories should regularly
report to physicians and provide the results of in vitro susceptibility
tests of antimicrobials used in their hospitals, which reflect the
susceptibility characteristics of hospital- and community-acquired
pathogens. These reports help doctors choose antimicrobials when
treating.
Dilution method
Minimum inhibitory concentrations (MICs) were determined by quantitative
methods, and these MIC values can be used to assess the sensitivity of
bacteria to antimicrobials. The MIC should be determined using standard
test methods, and the measured MIC values can be interpreted according
to the criteria in Table 1.
Paper diffusion method
The quantitative method of determining the diameter of the inhibition
zone can also be used to estimate the reproducibility of bacterial
susceptibility to antimicrobials. The size of the inhibition zone
represents the sensitivity of bacteria to antimicrobials and should be
determined using standard test methods. This method used paper
impregnated with 30 μg of ceftazidime to determine the sensitivity of
bacteria to antimicrobials, and the interpretation criteria of the paper
diffusion method are shown in Table 1.
Table 1. Interpretation criteria for susceptibility testing for ceftazidime
| Pathogenic bacteria Enterobacteriaceae§ |
Minimum inhibitory concentration (μg/ml). | The diameter of the inhibition zone (mm) of the paper diffusion method | ||||
| Sensitive ≤ 4 |
Intermediary 8 |
Drug resistance ≥16 |
Sensitive ≥ 21 |
Intermediary 18-20 |
Drug resistance ≤17 |
|
| Haemophilus influenzae a | ≤ 2 | - | - | ≥26 | - | - |
| Pseudomonas aeruginosa* | ≤ 8 | - | ≥16 | ≥18 | - | ≤ 17 |
§ Enterobacteriaceae
sensitivity interpretation criteria are based on a dose of 1 g per 8
hours. For mediator-sensitive isolates, patients with normal renal
function were administered a dose of 2 g every 8 hours.
*The sensitivity interpretation criteria for Pseudomonas aeruginosa are
based on a dose of 2 g intravenously every 8 hours in patients with
normal renal function.
aThere is currently no information on resistant strains other than the
"sensitive" category, and it is not possible to define a category other
than "sensitive". If a MIC result other than sensitive is detected, it
should be submitted to the reference laboratory for additional testing.
Staphylococcal sensitivity to ceftazidime may be derived from tests for
penicillin and cefoxitin or oxacillin alone.
The susceptibility report "sensitive" indicates that the concentration
typically achieved by antimicrobials at the site of infection is likely
to inhibit the growth of pathogens. Reporting "intermediary" indicates
that the result is ambiguous and should be repeated if the microorganism
is not completely sensitive to a replaceable clinically viable drug.
This classification implies that the drug may be clinically applicable
in parts of the body where it is physiologically aggregated or where
high doses can be used. This classification also provides a buffer to
prevent interpretive differences due to small, uncontrolled technical
factors. Reporting "resistance" means that the concentrations normally
achieved at the site of infection are likely not to inhibit the growth
of pathogens and other treatments should be used.
Quality control
Standardized drug susceptibility testing methods require laboratory
controls to monitor and ensure the accuracy and precision of the samples
and reagents used in the drug susceptibility test, as well as the
technique of the test operator. Ceftazidime standard powders should
provide the MIC value range in Table 2. For diffusion methods using 30
μg ceftazidime paper, the criteria in Table 2 should be met.
Table 2. Acceptable quality control ranges for ceftazidi
| Quality control strains | Minimum antibacterial concentration (μg/ml). | The diameter of the inhibition zone (mm) of the paper diffusion method |
| Escherichia coli ATCC 25922 | 0.06-0.5 | 25-32 |
| Staphylococcus aureus ATCC 25923 | --------- | 16-20 |
| Staphylococcus aureus ATCC 29213 | 4-16 | --------- |
| Haemophilus influenzae ATCC 49247 | 0.12-1 | 27-35 |
| Neisseria gonorrhoeae ATCC 49226 | 0.03-0.12 | 35-43 |
| Pseudomonas aeruginosa ATCC 27853 | 1-4 | 22-29 |
Toxicology Research
Genotoxicity
The results of ceftazidime mouse micronucleus test and Ames test were negative.
Reproductive toxicity
Reproductive toxicity studies have shown no damage to fertility and fetuses at 40 times the human dose in mice and rats.
Carcinogenicity
No long-term animal studies have been conducted to assess the potential carcinogenicity of ceftazidime.
[Storage]
Keep away from light, airtight, and store no more than 25°C.
[Packaging]
Packaged with medium borosilicate glass molded injection bottles,
sterile powder for injection with butyl bromide rubber stoppers and
aluminum-plastic combination caps for antibiotic bottles. 10
bottles/box.
[Validity period]
24 months
[Implementation standard] National Medical Products Administration standard YB H 13 912 023
[Approval number]
(1) Sinopharm quasi-character H20064883 (0.75g).
(2) Sinopharm quasi-word H20064884 (1.5g).
[Marketing authorization holder]
Name: Guangdong Jincheng Jinsu Pharmaceutical Co., Ltd
Registered address: No. 10, Shennong Road, Torch Development Zone, Zhongshan City, Guangdong Province
Postal code: 528437
Service hotline: 400-9988-970
Telephone number: (0760) 22830525 (switchboard).
Fax number: (0760) 22578279
Website: www.gdjcjs.com
[Manufacturer]
Company name: Guangdong Jincheng Jinsu Pharmaceutical Co., Ltd
Production address: No. 10 Shennong Road, Torch Development Zone, Zhongshan City, Guangdong Province
Postal code: 528437
Service hotline: 400-9988-970
Telephone number: (0760) 22830525 (switchboard).
Fax number: (0760) 22578279
Website: http://www.gdjcjs.com
-
Prev: Gestrinone