 CN
CN
Ceftriaxone Sodium for Injection
Instructions for Ceftriaxone Sodium for Injection
Please read the instructions carefully and use under the guidance of a physician
Warning: This product cannot be used in solutions containing calcium, such as Hartmann and Ringer.
Concomitant use of this product with calcium-containing agents or calcium-containing products may lead to adverse events that may lead to fatal outcomes.
[Name of the drug]
Generic name: Ceftriaxone Sodium for Injection
Product name: Ceftriaxone Sodium for Injection
Hanyu Pinyin: Zhusheyong Toubaoqusongna
[Ingredients]
The main ingredient of this product is ceftriaxone sodium.
The chemical name is: ( R6R,7 R )-7-[[(2Z Z)-(2-aminothiazol-4-yl)(methoxyimino)acetyl]amino]-3-[[(2-methyl-6-hydroxy-5-oxo-2,5-dihydro-1,2,4-triazine-3-)thio]methyl]-8- Oxo-5-thio-1-azobiabicyclic [4.2.0]oct-2-en-2-carboxylate disodium salt triple hemihydrate.
Chemical structural formula:
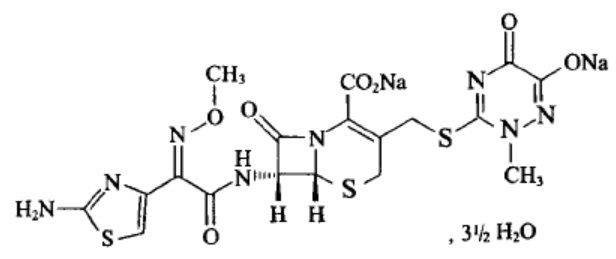
Molecular formula: C 18 H 16 N 8 Na 2 O 7 S 3 · 31/2H 2 O
Molecular weight: 661.59
[Characteristics]
This product is a white or white-like crystalline powder; Odorless.
[Indications]
Infections caused by pathogenic bacteria that are sensitive to this product, such as: sepsis; meningitis; Disseminated Lyme disease (early and late); abdominal infections (peritonitis, biliary and gastrointestinal infections); bone, joint, soft tissue, skin and wound infections; infection in patients with low immune mechanisms; Kidney and urinary tract infections; respiratory infections, especially pneumonia, ENT infections; infections of the reproductive system, including gonorrhea; Prevent infection before surgery.
[Specifications]
As C 6 p.m. :18 N 8 O 7 S 3 计 (1)0.5g (2)1.0g
[Usage and dosage]
Standard dosage
Adults and children over 12 years old: The usual dosage of this product is 1~2 grams once daily (every 24 hours).
In critical cases or infections caused by moderately sensitive bacteria, the dose can be increased to 4 grams once a day.
Newborns, infants and children under 12 years of age
It is recommended to use once daily at the following doses.
The daily dose for newborns (less than 14 days) is 20~50 mg/kg according to body weight, not more than 50 mg/kg, and ceftriaxone is contraindicated for correcting premature infants with a gestational age of less than 41 weeks (gestational age + actual age) (see [Contraindication]). The safety of use in neonates (those with a birth weight less than 2 kg) has not been established. Newborns with jaundice or with severe tendencies to jaundice should use this product with caution or avoid.
If the neonate (≤ 28 days) requires (or is expected to need) intravenous treatment with calcium-containing solutions, including continuous instillations of calcium-containing solutions (eg, parenteral nutrient solutions), ceftriaxone is prohibited due to the risk of ceftriaxone-calcium deposition (see Contraindications).
The daily dose for newborns, infants and children (15 days to 12 years old) is 20~80 mg/kg by body weight.
Children weighing 50 kg or more should use the usual adult dose.
Intravenous dosage should be at least 30 minutes for infants and children under 12 years of age when body weight is more than 50 mg/kg. Neonates should be given intravenous fluids for more than 60 minutes to reduce the potential risk of bilirubin encephalopathy.
Elderly patients
Unless elderly patients have severe renal function and liver impairment, the dose of ceftriaxone in elderly patients generally does not need to be adjusted.
Treatment
The course of treatment depends on the course of the disease. As with general antimicrobial therapy regimens, this product should be continued for at least 48 to 72 hours after the fever has subsided or evidence of bacterial clearance has been obtained.
Combination medication
Under test conditions, the synergistic effect of this product with aminoglycoside antimicrobials on many gram-negative bacilli has been demonstrated. Although the potential effects of this combination are not always predicted, the combination should be considered for serious, life-threatening infections such as Pseudomonas aeruginosa. Because ceftriaxone is chemically incompatible with aminoglycosides, the two drugs should be used separately when using the recommended dose.
Chemical incompatibility of ceftriaxone with amacridine, vancomycin, and fluconazole has also been observed when administered intravenously.
Special medication guidance
Meningitis: Infants and children with bacterial meningitis, start treatment at a dose of 100 mg per kg of body weight (not more than 4 g) once daily, and may be reduced as appropriate once the results of the pathogen and susceptibility test are confirmed, and the following courses of treatment have been shown to be effective:
Neisseria meningitidis for 4 days
Haemophilus influenzae 6 days
Streptococcus pneumoniae for 7 days
Lyme disease: children and adults should be given a maximum dose of 2 grams at 50 mg/kg by body weight once a day for 14 days.
Gonorrhea: For the treatment of gonorrhea (penicillinase-producing and non-penicillinase strains) The recommended dose of this product is a single dose of 250 mg intramuscularly.
Preoperative prophylactic medication: To prevent postoperative infection of contaminated or non-contaminated surgery, inject a single dose of 1~2 grams of this product 30~90 minutes before surgery according to the risk of infection. For colorectal surgery, this product has been shown to be effective when used alone or in combination with 5-nitroimidazole (such as ornidazole) (to be used separately, see [Dosage]).
Patients with renal impairment: Patients with renal impairment, if their liver function is not impaired, do not need to reduce the dosage of this product, only for patients with end-stage renal failure (creatinine clearance < 10 ml/min), the dosage of the daily product should not exceed 2 grams. Ceftriaxone cannot be cleared by peritoneal dialysis or hemodialysis. Patients on dialysis do not need to add additional doses after dialysis.
Patients with liver function impairment: Patients with liver function impairment do not need to reduce the dosage of this product if their kidney function is not impaired.
Patients with severe liver and kidney impairment: Patients with severe liver and kidney impairment are recommended for clinical safety and efficacy monitoring.
Medication method
The newly prepared solution can maintain its physical and chemical stability at room temperature for up to 6 hours, or in the refrigerator at 2~8°C for 24 hours, but according to the general principle, the prepared solution should be used immediately. Depending on its concentration and storage time, the solution appears pale yellow to amber. Solution color has no significance for drug effectiveness or tolerability.
Intramuscular injection: 0.25 grams or 0.5 grams of this product is dissolved in 2 ml of 1% lidocaine hydrochloride, and 1 gram is dissolved in 3.5 ml for intramuscular injection. Lidocaine solution should never be used intravenously (see Contraindications).
Intravenous injection: 0.25 grams or 0.5 grams of this product is dissolved in 5 ml of sterile injection water, and 1 gram is dissolved in 10 ml for intravenous injection, and the injection time cannot be less than 4 minutes.
Intravenous infusion: The intravenous infusion time is at least 30 minutes, and 2 grams of this product is dissolved in one of the following calcium-free intravenous solutions of 40 ml or more specifications, such as: 0.9% sodium chloride solution, 0.45% sodium chloride + 2.5% glucose injection, 5% glucose, 10% glucose, 5% glucose plus 6% dextran, 6~10% hydroxyethyl starch intravenous solution, sterilized water for injection. Due to the potential for incompatibility between drugs, this product should not be mixed with solutions containing other antibacterial drugs or added to them when infusion of other antibacterial solutions. It cannot be diluted in liquids other than those listed above.
[Adverse reaction]
Clinical trials
The most commonly reported adverse reactions of ceftriaxone are eosinophilia, leukopenia, thrombocytopenia, diarrhea, rash, and elevated liver enzymes.
Data used to determine the frequency of adverse drug reactions to ceftriaxone are derived from clinical trials.
The following conventions are used for frequency classification: very common (≥1/10), common (≥1/100~<1/10), uncommon (≥1/1000~<1/100), and rare (≥1/10000~<1/1000).
Table 1. List of adverse reactions
| Systemic organ classification | Common | Not common | Rare |
| Infections and infectious diseases | Genital fungal infections | Pseudomembranous colitis | |
| Diseases of the blood and lymphatic system | Eosinophilia Leukopenia Thrombocytopenia |
Agranulocytopenia Anemia Coagulopathy |
|
| Neurological disorders | Headache Dizziness |
||
| Respiratory, thoracic and mediastinal diseases | Bronchospasm | ||
| Diseases of the gastrointestinal system | Diarrhea Loose stool |
Nausea Vomiting |
|
| Diseases of the hepatobiliary system | Elevated liver enzymes | ||
| Skin and subcutaneous tissue disorders | Rash | Itching | Hives |
| Kidney and urinary system diseases | Hematuria Diabetes |
||
| Systemic disease and various reactions at the site of administration |
Phlebitis Pain at the injection site Fever |
Edema Shivering |
|
| Check | Blood creatinine is elevated |
After listing
The following adverse reactions were found during use after the marketing of ceftriaxone. The number of people reporting these reactions is unknown, so it is not always possible to reliably estimate their frequency and/or determine a causal relationship between them and drug exposure.
Systemic side effects
Gastrointestinal reactions: pancreatitis, stomatitis and glossitis.
Abnormal hematology tests: Isolated cases of agranulocytosis (<500/mm3) have been reported, most of which occur after 10 days of treatment at a total dose of more than 20 g.
Skin reactions: Separate cases of acute generalized exanthematous impetigo disease (AGEP) and severe skin reactions (erythema multiforme, Stevens Johnson syndrome, or Lyell syndrome/toxic epidermal necrolaxosis) have been reported.
Neurological disorders: convulsions
Infection and infectious diseases: double infection
Other rare side effects
Gallbladder symptomatic ceftriaxone calcium salt deposition, kernicterus, oliguria, and allergic or anaphylactolike reactions.
Interaction with calcium
Two in vitro studies evaluated the interaction of ceftriaxone with calcium, one using adult plasma and the other using neonatal umbilical cord plasma. The maximum concentration of ceftriaxone is 1 mM (more than the plasma concentration obtained by infusion of 2 g of ceftriaxone for more than 30 minutes), and the maximum calcium concentration is 12 mM (48 mg/dL). The recovery of ceftriaxone decreased when calcium concentrations in adult plasma were 6 mM (24 mg/dL) or higher, and decreased in ceftriaxone at neonatal plasma concentrations of 4 mM (16 mg/dL) or higher. This suggests possible ceftriaxone-calcium precipitate production.
A crystalline substance has been reported in the lungs and kidneys of newborns who have received this product and calcium-containing infusions during autopsy of a small number of deaths. In some cases, the same infusion tube was used to instill the product and calcium-containing fluids, and in some cases, sediment was seen in the tube. At least one death has been reported in newborns who were instilled with this product and calcium-containing infusion through different infusion tubes at different times; An autopsy of the newborn revealed no crystalline material. Similar reports have not been seen in other patients except neonates (see [Precautions]).
Cases of ceftriaxone deposit in the urethra have been reported, more often in children treated with high doses (eg, ≥80 mg/kg per day, or more than 10 g in total) and with other risk factors (eg, dehydration, bed rest, etc.). This event can be symptomatic or asymptomatic and causes ureteral obstruction and acute post-renal renal failure, but can usually be reversed with discontinuation.
Local side effects
In rare cases, phlebitis occurs after intravenous medication, which can be reduced by slowing down the rate of intravenous injection (2 to 4 minutes).
Examination: Coombs test false positive, galactosemia test false positive, non-enzymatic glucose test false positive.
[Contraindication]
Allergic reactions
Ceftriaxone is contraindicated in patients with known allergies to ceftriaxone, any of its excipients, or any other cephalosporins. People with a previous allergy to penicillin or other β-lactam drugs are at increased risk of developing an allergy to ceftriaxone (see Precautions).
Lidocaine
When using lidocaine solution as a solvent, contraindications to lidocaine must be ruled out before intramuscular administration of ceftriaxone (see Dosage). See the contraindications section of the lidocaine prescribing information. Ceftriaxone solutions containing lidocaine should never be administered intravenously.
Premature babies
Ceftriaxone is contraindicated for correcting preterm infants with a gestational age of less than 41 weeks (gestational age + chronological age).
Neonates with hyperbilirubinemia
Ceftriaxone should not be used for the treatment of neonatal hyperbilirubinemia. In vitro studies have shown that ceftriaxone can replace bilirubin and bind to serum albumin, leading to a possible risk of bilirubin encephalopathy in these patients.
Neonates are given calcium-containing intravenous fluids
If the neonate (≤ 28 days) requires (or is expected to need) the use of calcium-containing intravenous fluids, including calcium-containing intravenous infusions for treatment such as parenteral nutrition, this product is contraindicated due to the risk of ceftriaxone-calcium precipitate (see Dosage and Drug Interactions).
[Precautions]
Be vigilant
(1) This product should be administered under the guidance of a professional physician, and the hospital can take first aid measures for allergic reactions. Before using this product, it is necessary to inquire about the medical history in detail, and the inquiry should be targeted, including the history of allergy to penicillins, cephalosporins, any other drugs, allergic constitution (such as whether there is a history of anaphylactic shock, allergic asthma, allergic rhinitis, urticaria and other diseases), family history, etc. This product should be used with caution in patients with a history of allergy, especially to drugs, as see the contraindications section for drug contraindications. People with penicillin anaphylactic shock should not use cephalosporins. After taking the drug, especially within 30 minutes of the first dose, stay in the hospital for close observation, and if anaphylactic shock is found, it will be treated urgently in time. Like other cephalosporin antibiotics, allergic reactions have been reported to cause death, even if the patient has an unknown allergy history or has used this product.
(2) Co-infection: As with other antibacterial drugs, superinfection caused by microorganisms that are insensitive to ceftriaxone may occur after using ceftriaxone.
(3) Hemolytic anemia: Immune-mediated hemolytic anemia was observed in patients using cephalosporin antibiotics, including this product. Cases of severe hemolytic anemia, including death, have been reported in both adult and child treatment. If a patient develops anemia while on ceftriaxone therapy, ceftriaxone should be considered for cephalosporin-related anemia at diagnosis and ceftriaxone should be discontinued until the cause is established.
(4) Clostridium difficile diarrhea: Almost all antibiotics, including this product, have been reported with Clostridium difficile diarrhea (CDAD), which may be mild diarrhea to fatal colitis depending on the severity of the disease. Antibiotic therapy alters the normal flora of the colon, leading to an overgrowth of C. difficile.
Clostridium difficile produces toxins A and B, and toxins A and B promote the development of CDAD. High-yielding strains of C. difficile toxin increase morbidity and mortality because these infections are resistant to antibiotics and may require colon resection. All patients with diarrhea after antibiotic use must consider the possibility of CDAD. Careful history is required as CDAD has been reported to develop after two months of antibiotic therapy.
If CDAD is suspected or diagnosed, it may be necessary to discontinue the antibiotic being used that has no effect on Clostridium difficile. Appropriate balanced fluid and electrolyte treatment, protein supplementation, antibiotic therapy for C. difficile, and surgical evaluation according to clinical conditions.
(5) Because this product will cause adverse reactions to the gastrointestinal system such as diarrhea, loose stools, and pseudomembranous colitis like other cephalosporins, people with a history of gastrointestinal diseases should closely observe the changes in their condition when intravenous infusion of this product.
(6) Calcium-ceftriaxone precipitation: Calcium-ceftriaxone precipitation has been observed in the gallbladder in ultrasound scan in patients treated with ceftriaxone, especially at doses of 1g or more per day. The probability of such precipitation appears to be highest in pediatric patients. After cesftriaxone treatment, the sediment disappears and rarely accompanied by symptoms. Conservative nonsurgical treatment is recommended for patients with these co-symptoms, and the clinician should consider whether to discontinue ceftriaxone based on an individual benefit-risk assessment.
In the known scientific data, no intravascular precipitation has been reported in patients treated with ceftriaxone and calcium-containing solutions or products at the same time, except in neonates. However, ceftriaxone should not be mixed with or concomitantly used with calcium-containing solutions, regardless of the patient, even through a different infusion line (see Contraindications for information on neonates).
(7) Pediatrics: The safety and effectiveness of this product for newborns, infants and children have been clarified in the [Usage and Dosage] section. Studies have shown that, like other cephalosporin antibiotics, ceftriaxone also replaces bilirubin from serum albumin. This product should not be used in neonates (especially premature infants) who may develop bilirubin encephalopathy (see [Contraindications]).
(8) Blood monitoring: Regular complete blood count should be performed during long-term treatment.
(9) Pancreatitis: Rare cases of pancreatitis (possibly caused by bile duct obstruction) have been reported in patients using ceftriaxone. Most of these patients have risk factors for cholestasis or sedimentary gallstones, such as prior high-risk therapy (major surgery), critical illness, and total parenteral nutrition, but ceftriaxone cannot be ruled out as a trigger or cofactor for bile deposition.
Substance abuse and dependence
Not applicable
The ability to drive and use machines
Adverse effects (e.g., dizziness) may occur during treatment with ceftriaxone, which may affect the ability to drive and use machinery (see Adverse Effects). Patients should be cautious when driving or operating machinery.
Impact on diagnostic tests
In patients treated with ceftriaxone, the Coombs test result may be false positive. Like other antibiotics, ceftriaxone can cause false positive results in galactosemia tests.
Similarly, non-enzymatic determination of urine glucose can also result in false positives. Therefore, during the use of ceftriaxone, urine glucose should be determined enzymatically.
In the presence of ceftriaxone, certain blood glucose tests may give falsely low blood glucose estimates. See instructions for each method. Alternative testing methods should be used if necessary.
[Medication for pregnant and lactating women]
Pregnant and lactating women must weigh the pros and cons of medication.
Ceftriaxone can cross the placental barrier. Safety in human pregnancy has not been established. Animal reproduction studies have not shown embryotoxicity, fetal toxicity, teratogenicity, or adverse effects on fertility, childbirth or perinatal period, and postnatal development in male or female animals. No embryotoxicity or teratogenicity has been seen in primate studies.
Ceftriaxone is excreted in small amounts in human milk. Breastfeeding women should be cautious in their medication.
[Children's medication]
The safety of use in neonates (those with a birth weight less than 2 kg) has not been established. The method of administration for newborns, infants and children has been clarified in the [Dosage] section. Ceftriaxone should not be used to treat neonates with hyperbilirubinemia. Do not use in neonates who may develop bilirubin encephalopathy (especially premature infants). Newborns with jaundice or with severe tendencies to jaundice should use this product with caution or avoid.
[Medication for the elderly]
Unless elderly patients have severe renal function and liver impairment, the dose of ceftriaxone in elderly patients generally does not need to be adjusted.
[Drug Interactions]
To date, no renal impairment has been found with the concomitant use of high doses of this product with strong diuretics such as furosemide.
There is conflicting evidence for the possible increase in nephrotoxicity of aminoglycosides when aminoglycosides are combined with cephalosporins. In these cases, the recommended monitoring of aminoglycoside blood concentrations and renal function in clinical practice should be strictly followed.
No disulfiram-like side effects have been found in drinkers after ceftriaxone administration. Because ceftriaxone does not contain an N-methylthiotracolium group, which may cause hemorrhagic problems with intolerance to ethanol and certain cephalosporin antibiotics.
The clearance of this product is not affected by probenecid. In vitro trials found that chloramphenicol in combination with ceftriaxone produced antagonistic effects.
Do not reconstitute this product with calcium-containing dilutions such as Ringer's or Hartmann's solutions or administer intravenously after further dilution of the complex, as this may result in precipitate. This product may also produce ceftriaxone-calcium precipitate when mixed with calcium-containing solutions in the same infusion tube. This product should not be administered concurrently with calcium-containing intravenous fluids, including calcium-containing injections (eg, parenteral nutrient solutions) continuously instilled through the Y-interface. However, other patients except neonates may receive sequential administration of this product and calcium-containing infusions, and the infusion tube must be thoroughly flushed with compatible fluids between infusions. In vitro studies using adult plasma and neonatal cord plasma demonstrated a higher risk of ceftriaxone-calcium preservites in neonates (see Dosage and Contraindications).
Concomitant use of ceftriaxone with vitamin K antagonists may increase the risk of bleeding. During and after ceftriaxone treatment, coagulation function should be monitored frequently, and anticoagulant doses should be adjusted accordingly (see [Adverse Effects]).
Chemical incompatibility with amacridine, vancomycin and fluconazole has also been observed when administered intravenously.
[Drug overdose]
In the event of drug overdose, hemodialysis or peritoneal dialysis will not reduce blood concentration, and there is no special antidote, so symptomatic treatment should be given.
[Pharmacology and Toxicology]
Pharmacological effects
Ceftriaxone is a fungicide that works by inhibiting bacterial cell wall synthesis and is active in the presence of certain β-lactamases (including penicillinase and cephalosporinase) in gram-positive and gram-negative bacteria.
The main mechanisms of ceftriaxone resistance were hydrolysis of β-lactamase, changes in penicillin-binding proteins (PBPs), and decreased membrane permeability.
Interactions with other antimicrobials:
In vitro studies, the combination of chloramphenicol and ceftriaxone has an antagonistic effect.
In vitro and clinical infection, ceftriaxone is effective against most of the following bacteria (see [Indications]).
● Gram-negative bacteria
Acinetobacter calcium acetate
Enterobacteria aerogeniens
Enterobacteriaceae claugua
Escherichia coli
Haemophilus influenzae
Haemophilus parainfluenzae
Klebsiella
Klebsiella pneumoniae
Moraxella catarranger
Morganella Morse
Neisseria gonorrhoeae
Neisseria meningitidida
Proteus
Proteus vulgaris
Pseudomonas aeruginosa
Serratia marcescens
● Gram-positive bacteria
Staphylococcus aureus
Staphylococcus epidermidis
Streptococcus pneumoniae
Streptococcus pyogenes
Streptococcus grass greener
● Anaerobic bacteria
Bacteroides fragility
Clostridium spp
Digestive Streptococcus
The following in vitro trial data are available, but their clinical significance is unclear. At least 90% of the following microorganisms have a minimum in vitro inhibitory concentration (MIC value) less than or equal to the sensitive breakpoint of ceftriaxone. However, data on the effectiveness of ceftriaxone in the treatment of clinical infections caused by these microorganisms have not been obtained in adequate and well-controlled clinical trials.
● Gram-negative bacteria
Citrate heteroformis
Citrate freundii
Providence fungi
Salmonella genus (including Salmonella typhi).
Shigella genus
● Gram-positive bacteria
Streptococcus lactate
● Anaerobic bacteria
Produces Melanin Porphyromonas (Bacteroidetes).
Prevobacteria dilu (Bacteroidetes).
Sensitivity test method
Where possible, clinical microbiology laboratories should regularly report to physicians and provide the results of in vitro susceptibility tests of antimicrobials used in their hospitals, which reflect the susceptibility characteristics of hospital- and community-acquired pathogens. These reports help doctors choose antimicrobials when treating.
Dilution method
Minimum inhibitory concentrations (MICs) are determined by quantitative methods, and these minimum inhibitory concentration values can be used to assess the sensitivity of bacteria to antimicrobials. MIC should be determined using a standard test method (broth or agar) and the determined MIC values can be interpreted according to the criteria in Table 2.
Diffusion method
The quantitative method of determining the diameter of the inhibition zone can also be used to estimate the reproducibility of bacterial susceptibility to antimicrobials. The size of the bacteriological zone represents the sensitivity of the bacteria to antimicrobials and should be determined using standard test methods. The susceptibility of bacteria to antimicrobials was determined using paper plates impregnated with 30 μg of ceftriaxone, and the diffusion of paper was determined according to the criteria in Table 2.
Anaerobic method
For anaerobic bacteria, the minimum inhibitory concentration (MIC) of the ceftriaxone susceptibility test can be detected by standard agar diffusion method. The minimum antibacterial value obtained should be determined according to the criteria in Table 2.
Table 2: Sensitivity test interpretation criteria for ceftriaxone
| Pathogenic bacteria | Minimum inhibitory concentration (mg/L). | Diameter of the inhibition zone (mm). | ||||
| Sensitive (S). | Intermediary (I). | Drug resistance (R). | Sensitive (S). | Intermediary (I). | Drug resistance (R). | |
| Enterobacteriaceae a | ≤ 1 | 2 | ≥ 4 | ≥ 23 | 20~22 | ≤ 19 |
| Haemophilus influenzae b, c | ≤ 2 | - | - | ≥ 26 | - | - |
| Neisseria gonorrhoeaeaea | ≤ 0.25 | - | - | ≥ 35 | - | - |
| Neisseria meningitidis c | ≤ 0.12 | - | - | ≥ 34 | - | - |
| Streptococcus pneumoniae D meningitis isolate strain | ≤ 0.5 | 1 | ≥ 2 | - | - | - |
| Streptococcus pneumoniae D non-meningitis isolate | ≤ 1 | 2 | ≥ 4 | - | - | - |
| Streptococcus β-hemolytic group c |
≤ 0.5 | - | - | ≥ 24 | - | - |
| Streptococcus grass greener | ≤ 1 | 2 | ≥ 4 | ≥ 27 | 25~26 | ≤ 24 |
| Anaerobic bacteria (agar method). | ≤ 1 | 2 | ≥ 4 | - | - | - |
a The sensitivity explanation criteria for Enterobacteriaceae are based on 1 g IV every 24 hours. For moderately sensitive isolates, patients with normal renal function were given 2 g intravenously every 24 hours.
b The criteria for interpreting sensitivity to Haemophilus influenzae are based on 2 g of IV infusion every 24 hours in patients with normal renal function.
c Lack of available data on resistant organisms other than "sensitive" results. If the isolates show MIC results other than "sensitive", they should be sent to a reference laboratory for additional testing.
d Paper diffusion is not suitable for testing the susceptibility of Streptococcus pneumoniae to ceftriaxone. However, pneumococci > 20 mm in diameter from the oxacillin zone are sensitive to penicillin (MIC≤0.06 mg/L). The diameter of the oxacillin inhibition zone ≤19 mm cannot be used to determine the resistance or mediation of Streptococcus pneumoniae to penicillins (ceftriaxone).
Staphylococcal sensitivity to ceftriaxone may be inferred from tests of penicillin and cefoxitin/oxacillin.
The drug sensitivity report "sensitive" means that if the antimicrobial reaches an effective concentration at the site of infection, the growth of pathogenic bacteria will be largely inhibited. Reporting "intermediary" indicates that the result is ambiguous and should be repeated if the microorganism is not completely sensitive to a replaceable clinically viable drug. This classification implies possible clinical applicability in parts of the body where the drug is physiologically aggregated or where high doses can be used. This classification also provides a buffer to prevent interpretive differences due to small, uncontrolled technical factors. The report "resistance" means that if the antimicrobial can reach effective concentrations at the site of infection and cannot inhibit the growth of the pathogen to a large extent, other treatments should be taken.
Quality control:
Standardized drug susceptibility testing methods require laboratory controls to monitor and ensure the accuracy and precision of the samples and reagents used in the drug susceptibility test, as well as the technique of the test operator.
A ceftriaxone powder standard with the MIC values in Table 3 should be provided. For 30 μg ceftriaxone sheets using the diffusion method, the antibacterial diameter circle standard should be in line with the values in Table 3.
Table 3: Acceptable quality control ranges for ceftriaxone
| Quality control strains | Minimum inhibitory concentration (mg/L). | Diameter of the inhibition zone (mm). |
| Escherichia coli ATCC 25922 | 0.03-0.12 | 29-35 |
| Staphylococcus aureus ATCC 25923 | --- | 22-28 |
| Staphylococcus aureus ATCC 29213 | 1-8 | --- |
| Haemophilus influenzae ATCC 49247 | 0.06-0.25 | 31-39 |
| Neisseria gonorrhea ATCC 49226 | 0.004-0.015 | 39-51 |
| Pseudomonas aeruginosa ATCC 27853 | 8-64 | 17-23 |
| Streptococcus pneumoniae ATCC 49619 | 0.03-0.12 | 30-35 |
| Bacteroides fragilis ATCC 25285 (agar method). | 32-128 | --- |
| Bacteroides ATCC 29741 (agar method). | 64-256 | --- |
Toxicology Research
Genotoxicity
The results of ceftriaxone Ames test, micronucleus test, and chromosomal aberration test of cultured human lymphocytes in vitro were all negative.
Reproductive toxicity
Intravenous administration of ceftriaxone 586mg/kg/day (about 20 times the clinically recommended dose of 2g/day) had no effect on fertility.
Reproductive toxicity tests showed no embryotoxicity, fetal toxicity and teratogenicity in mice and rats at 20 times the usual human dose. No embryotoxicity or teratogenicity was observed in non-human primates at about 3 times the human dose.
In the Stage I (fertility and general reproductive toxicity) and III (perinatal toxicity) studies, intravenous ceftriaxone 586 mg/kg/day or less in rats had no significant effect on various reproductive indicators (including postpartum development, functional behavior, and offspring fertility) during pregnancy and lactation.
Other toxicities
Dogs (100 mg/kg/day for 4 weeks) and baboons (≥335 mg/kg/day for 6 weeks) were found to have ceftriaxone granular calcium salt deposition in the gallbladder bile. The incidence of this phenomenon is relatively low in humans, because ceftriaxone has a longer plasma half-life in humans, ceftriaxone calcium salts are more soluble in human gallbladder bile, and the calcium content in human gallbladder bile is relatively low.
[Pharmacokinetics]
The pharmacokinetics of ceftriaxone are nonlinear and, if based on total drug concentrations, all basic pharmacokinetic parameters, except for clearance half-lives, are dose-dependent and lower than the proportion of dose increases. Nonlinearity is due to plasma protein-binding saturation, so nonlinearity of total plasma ceftriaxone is observed, while nonlinearity of free (unbound) ceftriaxone is observed.
Absorb
The highest blood concentration is about 81 mg/L 2~3 hours after intramuscular injection of 1 gram of ceftriaxone. The area under the plasma concentration-time curve after intramuscular injection is equal to that after intravenous injection at the same dose, suggesting that the bioavailability of intramuscular ceftriaxone can reach 100%.
After intravenous bolus of 500 mg and 1 g of ceftriaxone, the mean peak blood medication of ceftriaxone was about 120 and 200 mg/L, respectively. After intravenous infusion of 500 mg, 1 g, and 2 g of ceftriaxone, the blood levels of ceftriaxone were approximately 80, 150, and 250 mg/L, respectively. After intramuscular injection, the mean peak blood medication of ceftriaxone is about half that of intravenous administration at the same dose.
distribution
The volume of distribution of ceftriaxone is 7~12 liters. After using 1~2 grams of ceftriaxone at a time, it shows good tissue and fluid penetration. In more than 60 tissues and body fluids such as lungs, heart, biliary tract, liver, tonsils, middle ear and nasal mucosa, bones, cerebrospinal fluid, pleural fluid, prostate fluid and synovial fluid, the drug concentration is maintained higher than the minimum inhibitory concentration of infected pathogenic bacteria for more than 24 hours. Intravenous ceftriaxone can quickly diffuse into the interstitial fluid and maintain a bactericidal concentration against sensitive bacteria for up to 24 hours.
Protein binding
Ceftriaxone binds reversibly to albumin, with a plasma protein binding rate of 95% at plasma concentrations below 100 mg/L L. The binding is saturated, and the binding ratio decreases with increasing concentration (up to 85% at plasma concentrations of 300 mg/L).
Penetration of special tissues
Ceftriaxone penetrates the meninges. The penetration rate is highest when the meninges are inflamed. Ceftriaxone has been reported to have an average peak concentration of 25% of plasma levels in ceftriaxone in patients with bacterial meningitis and 2% of plasma levels in patients without meningeal inflammation. The concentration of cerebrospinal fluid reaches its peak after 4~6 hours of intravenous injection.
Ceftriaxone penetrates the placenta and is secreted in small amounts in milk.
Metabolism
Ceftriaxone is not catabolized in the body, but is only converted into inactive metabolites by the intestinal flora.
Clear
The total plasma clearance was 10~22 ml/min. Renal clearance is 5~12 ml/min.
50%~60% of ceftriaxone is secreted in the urine in its original form, while 40%~50% is secreted in bile in its original form. The clearance half-life for adults is about 8 hours.
Pharmacokinetics in special populations
children
Ceftriaxone half-life is prolonged in neonates. From birth to 14 days of age, factors such as decreased glomerular filtration rate and altered protein binding rate may further increase free ceftriaxone levels. The half-life of childhood is lower than that of newborns or adults.
The total ceftriaxone plasma clearance and volume of distribution in neonates, infants, and children were greater than in adults.
Elderly
The average clearance half-life of the elderly over 75 years old is usually 2~3 times that of young people.
Patients with hepatic or renal impairment
In patients with hepatic or renal insufficiency, ceftriaxone has minimal changes in pharmacokinetics and only a slight increase in clearance half-life (less than twice), even in patients with severe renal impairment.
A small increase in the half-life of patients with renal impairment may be explained by an increase in compensated nonrenal clearance due to a decrease in protein binding and a corresponding increase in nonrenal clearance of total ceftriaxone.
In patients with hepatic impairment, the clearance half-life of ceftriaxone is not extended due to compensatory increases in renal clearance. Another reason is an increase in plasma free ceftriaxone, resulting in an abnormal increase in the observed total drug clearance and a parallel increase in the volume of distribution with the total clearance.
[Storage]
Shaded, airtight, and stored at no more than 30°C.
[Packaging]
Medium borosilicate glass injection bottle + sterile powder for injection is packaged with partially coated Teflon film and aluminum and plastic combination lid for antibiotic bottles. (1) 1 bottle per box (2) 10 bottles per box.
[Validity] 36 months
【Implementation Standards】 The National Medical Products Administration YBH02462021 standards
【Approval number】 Sinopharm quasi-H20043827 (0.5g).
Sinopharm standard word H20043825 (1.0g).
[Drug marketing authorization holder]
Company name: Guangdong Jincheng Jinsu Pharmaceutical Co., Ltd
Registered address: No. 10, Shennong Road, Torch Development Zone, Zhongshan City, Guangdong Province
[Manufacturer]
Company name: Guangdong Jincheng Jinsu Pharmaceutical Co., Ltd
Production address: No. 10 Shennong Road, Torch Development Zone, Zhongshan City, Guangdong Province
Postal code: 528437
Service hotline: 400-9988-970
Telephone number: (0760) 22830525 (switchboard).
Fax number: (0760) 22578279
Website: http://www.gdjcjs.com