 CN
CN
Cefazolin Sodium for Injection
Instructions for Cefazolin Sodium for Injection
Please read the instructions carefully and use under the guidance of a physician
Warning: This product is contraindicated in individuals who are allergic
to cephalosporins and those with a history of penicillin anaphylactic
shock or immediate reactions
[Name of the drug]
Generic name: Cefazolin Sodium for Injection
Product name: Cefazolin Sodium for Injection
Hanyu Pinyin: Zhusheyong Toubaozuolinna
[Ingredients]
The main ingredient of this product is cefazolin sodium.
Chemical Name: (6 R R,7 R )-3-[[(5-methyl-1,3,4-thiadiazole-2-yl)thio]methyl]-7-[(1 H H-tetraazole-1-yl)acetylamino]-8-oxo-5-thio-1-zabicyclic [4.2.0] Sodium oct-2-en-2-carboxate salt anhydride.
Chemical structural formula:
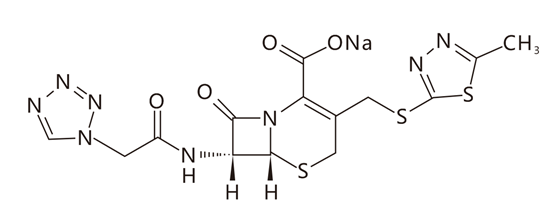
Molecular formula:C 14 H 13 N 8 NaO 4 S 3
Molecular weight: 476.48
[Characteristics]
This product is a white or white-like powder or crystalline powder; Odorless.
[Indications]
It is suitable for the treatment of the following infections caused by sensitive bacteria:
1. Respiratory tract infections: Respiratory tract infections caused by
Streptococcus pneumoniae, Klebsiella spp., Haemophilus influenzae,
Staphylococcus aureus (penicillin-sensitive and penicillin-resistant),
and group A β-hemolytic streptococcus, including otitis media,
bronchitis, pneumonia, etc.
2. Urinary tract infections: Urinary tract infections caused by
Escherichia coli, Proteus mirabacterium, Klebsiella spp. and some
bacteria of the genus Enterobacteriaceae and Enterococcus.
3. Skin and soft tissue infections: Skin and soft tissue infections
caused by Staphylococcus aureus (penicillin sensitive and penicillin
resistant), group A β-hemolytic streptococcus and other streptococci
bacteria.
4. Bone and Joint Infections: Bone and joint infections caused by Staphylococcus aureus.
5. Sepsis: Sepsis caused by Streptococcus pneumoniae, Staphylococcus
aureus (penicillin-sensitive and penicillin-resistant), Proteus mira,
Escherichia coli and Klebsiella spp.
6. Infective endocarditis: Infective endocarditis caused by
Staphylococcus aureus (penicillin-sensitive and penicillin-resistant)
and group β-hemolytic streptococcus.
7. Hepatobiliary system infection: Hepatobiliary system infection caused
by Escherichia coli, various streptococcus spp., Proteus mirabyl,
Klebsiella spp. and Staphylococcus aureus.
8. Reproductive system infections: Reproductive system infections (such
as prostatitis, epididymitis) caused by Escherichia coli, Proteus
mirabacter, Klebsiella spp. and some enterococci.
9. Perioperative infection prevention: This product can also be used as a
prophylactic drug before, during and after surgery. Reduces the
incidence of certain postoperative infections in contaminated or
potentially contaminated patients (e.g., vaginal hysterectomy and
cholecystectomy surgery, over 70 years of age, with acute cholecystitis,
obstructive jaundice, or high risk of common bile duct stones).
Perioperative use of this product may also be effective in preventing
the risk of serious infection of the surgical site during surgery (e.g.,
during open-heart surgery and joint replacement).
Prophylactic administration of this product should usually be
discontinued within 24 hours of surgical procedure. During surgery, if
an infection may lead to serious consequences (e.g., open-heart surgery
and joint replacement), this product can be continued prophylactically
for 3 to 5 days after surgery is completed.
This product should not be used for central nervous system infections.
It is less effective for chronic urinary tract infections, especially
those with abnormal urinary tract anatomy. This product is not suitable
for the treatment of gonorrhea and syphilis.
[Specifications]
As C 2 p.m. :14 N 8 O 4 S 3 计 1.0g
[Usage and dosage]
1. Adult medication
Intravenous slow bolus, intravenous infusion or intramuscular injection,
0.5g~1g at a time, 2~4 times a day, severe infection can be increased
to 6g a day, divided into 2~4 intravenous injections. The recommended
dose is shown in Table 1. Intravenous (IV) administration should be no
less than 30 minutes.
| Table 1 Creatinine clearance ≥ 55ml/min recommended dose for adult patients | ||
| Type of infection | Dosage | Frequency |
| Moderate to severe infection | 500mg~1g | Every 6~8 hours |
| Mild infection caused by gram-positive sensitive bacteria | 250mg~500mg | Every 8 hours |
| Acute, simple urinary tract infection | 1g | Every 12 hours |
| Pneumococcal pneumonia. | 500mg | Every 12 hours |
| Serious and life-threatening infections (e.g., endocarditis, sepsis, etc.)* | 1g~1.5g | Every 6 hours |
*In rare cases, patients should be treated with cefazolin up to 12 g per day.
2. Perioperative infection prevention medication
To prevent postoperative infection after contaminated or potentially contaminated surgery, the recommended dose is:
. 1g~2g intravenously administered 0.5~1 hour before surgery.
. For prolonged surgical procedures (e.g., 2 hours or more),
intraoperative intravenous administration of 500 mg to 1 g (adjust the
dosage according to the duration of the surgical procedure).
. Within 24 hours after surgery, 500mg~1g was administered intravenously every 6~8 hours.
Important:
(1) Preoperative dose is given before the start of surgery (0.5~1 hour)
so that the concentration of antibiotics in serum and tissue reaches
sufficient when the surgical incision is started;
(2) If necessary, cefazolin is given at appropriate intervals during
surgery to ensure adequate antibiotic concentrations at the expected
moment of maximum exposure to the source of infection.
Prophylactic administration of cefazolin should usually be stopped
within 24 hours after surgery. If an infection that may lead to serious
consequences occurs during surgery (eg, open-heart surgery and joint
replacement), cefazolin may be continued prophylactically for 3~5 days
after surgery.
3. Medication for patients with renal insufficiency
When cefazolin is used in patients with renal insufficiency, the dose
needs to be adjusted, see table 2. The recommended dose reduction should
be given after the first dose (depending on the severity of the
infection).
| Table 2 Dose adjustment in patients with renal insufficiency | ||
| Creatinine clearance | Dosage | Frequency |
| ≥55ml/min | Full dose | Normal dosing frequency |
| 35~54ml/min | Full dose | Every 8 hours or more |
| 11~34ml/min | 1/2 regular dose | Every 12 hours |
| ≤10ml/min | 1/2 regular dose | Every 18~24 hours |
If the creatinine clearance
rate of patients with renal dysfunction is greater than or equal to 55
ml/min, the normal dose can still be administered. When the creatinine
clearance rate is 35~54ml/min, the full dose can be given, but the
dosing interval should be at least 8 hours; When the creatinine
clearance rate is 11~34ml/min, give 1/2 of the regular dose every 12
hours; When the creatinine clearance rate is less than or equal to
10ml/min, give 1/2 of the regular dose every 18~24 hours. All patients
with varying degrees of renal impairment should have their starting
loading dose adjusted according to the severity of infection. Patients
undergoing peritoneal dialysis; See Pharmacokinetics.
4. Medication for children
For infants and children over 1 month old, for the vast majority of
children with mild and moderate infection, according to their body
weight of 25~50mg/kg every day, 3~4 intravenous slow bolus, intravenous
drip or intramuscular injection; For children with severe infections,
the daily dose can be increased to 100 mg/kg.
The safety of this product in premature infants and neonates has not
been established, so this product is not recommended for premature
infants and neonates. In children with mild to moderate renal
insufficiency (creatinine clearance rate of 70~40ml/min), 60% of the
normal dose is given every 12 hours.
In pediatric patients with moderate renal insufficiency (creatinine
clearance of 40~20ml/min), 25% of the normal dose is given every 12
hours. In pediatric patients with severe renal insufficiency (creatinine
clearance rate of 20~5ml/min), 10% of the normal dose is given every 24
hours. The recommended dose reduction should be given after the first
dose.
[Adverse reaction]
The following adverse reactions have been reported:
Skin and subcutaneous tissue: rash, itching, hyperhidrosis, flushing,
angioedema, allergic purpura, urticaria, erythema multiforme,
exfoliative dermatitis, Stevens-Johnson syndrome, toxic epidermal
necrolysis, acute generalized eruptive pustular dermatosis.
Digestive system: oral candidiasis (oral thrush), dry mouth, bitter
mouth, mouth ulcers, nausea, vomiting, stomach cramps, abdominal pain,
bloating, diarrhea, constipation, hepatitis, jaundice, anorexia and
pseudomembranous colitis. Pseudomembranous colitis may occur during or
after antibiotic therapy. Transient elevations in serum aminotransferase
(SGOT, SGPT) and alkaline phosphatase levels are seen. Rarely, nausea
and vomiting.
Systemic and administration site reactions: drug fever (occasionally),
chest discomfort, fatigue, rarely thrombophlebitis occurring
intravenously, rash, itching and swelling at the injection site.
Occasional pain at the injection site after intramuscular injection
administration, and some induration occurred. They are less and lighter
than cefothiophene.
Immune system: anaphylaxis (incidence 1.1%), hypersensitivity reaction, anaphylactic shock.
Mental and nervous system: dizziness, headache, general or local
numbness, tremors, tingling sensations in the skin, syncope, increased
intracranial pressure, convulsions, convulsions, drowsiness,
restlessness, insomnia, hallucinations, nightmares, vertigo, hot
flashes.
Respiratory system: dyspnea, pleural effusion, laryngeal edema, cough,
rhinitis, bronchospasm, interstitial pneumonia, eosinophilic pneumonia.
Cardiovascular system: palpitations, cyanosis, tachycardia, atrial
fibrillation and other arrhythmias, decreased blood pressure, increased
blood pressure.
Hematological system: coagulation dysfunction, neutropenia, leukopenia,
thrombocytopenia, thrombocytosis, pancytopenia, basophilia,
eosinophilia, agranulocytosis, eosinophilia (incidence of 1.7%),
leukocytosis, granulocytosis, mononucleosis, anemia, aplastic anemia,
hemolytic anemia.
Kidney and urinary system: hematuria, urinary incontinence, elevated BUN
value, elevated serum creatinine, interstitial nephritis, renal
failure. Patients with renal insufficiency may experience
encephalopathic reactions such as confusion and seizures when using high
doses (12g per day) of this product.
Other: eyelid edema, dry eyes, blurred vision, arthralgia, muscle
weakness, myalgia, tinnitus. Itching of the genitals and anus (including
vulvar itching, genital tumors, and vaginitis). Candida albicans double
infection is occasional.
[Contraindication]
1. Contraindicated for those who are allergic to cefazolin.
2. It is prohibited for those who are allergic to other cephalosporins.
3. It is contraindicated in patients with a history of severe allergy to penicillin or other β-lactams.
[Precautions]
1. Cross-allergic reaction: Patients who are allergic to one
cephalosporin or cephamycin may also be allergic to other cephalosporins
or cephalomycins; Patients who are allergic to penicillin, penicillin
derivatives, or penicillamine may also be allergic to cephalosporins or
cephalomycin.
Before using this product, patients must be asked in detail whether they
have a history of prior allergy to cefazolin, other cephalosporins,
penicillins, or other drugs. This product should not be used if there is
a history of anaphylactic shock with penicillins. If an allergic
reaction occurs during the course of treatment, the drug should be
stopped immediately. In the event of anaphylactic shock, emergency
measures such as epinephrine, glucocorticoids and antihistamines should
be kept open, oxygen inhaled, and administered.
2. Interference with diagnosis: 1% of patients treated with cefazolin
may have a positive direct or indirect antiglobulin Coombs test and
false positive urine glucose (copper sulfate method). A small number of
patients may have elevated alkaline phosphatase and serum
aminotransferase.
3. For patients with renal insufficiency:
Patients with low urine output due to impaired or renal insufficiency
should use this product with caution, and the amount must be reduced
when applying. As with other β-lactam antibiotics, seizures can occur if
inappropriately high doses are given to patients with impaired renal
function (creatinine clearance less than 55 mL/min).
4. Patients with hepatic impairment, renal impairment, or malnutrition,
patients with a longer course of treatment, and patients who have been
stable on anticoagulation therapy may be at risk of cefazolin-related
decreased prothrombin activity.
5. Long-term use can lead to the overgrowth of bacteria resistant to
this product, and appropriate measures should be taken in time once a
second infection occurs during treatment.
6. As with all cephalosporins, this product should be used with caution
in patients with gastrointestinal disorders, especially those with a
history of colitis.
7. Clostridium difficile associated diarrhea (CDAD) has been reported in
almost all antimicrobials, including cefazolin, ranging in severity
from mild diarrhea to fatal colitis. Antimicrobial therapy alters the
normal flora in the patient's colon, leading to an overgrowth of C.
difficile.
Toxins A and B produced by Clostridium difficile are responsible for the
occurrence of CDAD. Strains of Clostridium difficile that produce high
levels of toxins can cause increased morbidity and mortality of CDAD,
and because these infections are antimicrobial-refractory, colectomy may
be necessary in such patients. Anyone who develops diarrhea after
antibiotics must consider the possibility of developing CDAD. CDAD has
been reported to occur 2 months after the end of antimicrobial therapy,
so it is necessary to carefully understand the patient's medical history
when performing CDAD differentiation.
Once CDAD is suspected or confirmed, the antibiotic the patient is
receiving may need to be discontinued (except for antibiotics that have a
direct inhibitory effect on Clostridium difficile). Patients should
also be evaluated surgically for appropriate fluid and electrolyte
management, protein supplementation, antibiotic treatment for C.
difficile infection, and surgical evaluation as clinically indicated.
8. This product is compatible with the following drugs and is
contraindicated and cannot be dripped in the same bottle: amikacin
sulfate, kanamycin sulfate, chlortetracycline hydrochloride,
oxytetracycline hydrochloride, erythromycin gluconate, polymyxin sulfate
B, colistin sodium mesylate sodium, calcium gluconate.
[Medication for pregnant and lactating women]
Pregnant women
Animal reproduction studies have been conducted in rats, mice, and
rabbits, and there is no evidence of impairment of fetal or fetal
fertility due to cefazolin when given up to 25 times the human dose.
However, there have been no adequate and well-controlled studies in
pregnant women. Because animal reproductive testing does not always
predict human response, this product should only be used when clearly
needed.
Cefazolin is used before cesarean section, and the drug concentration in
the umbilical cord blood is about 1/4~1/3 of the maternal drug
concentration. This product does not appear to have adverse effects on
the fetus.
Lactating women
The content in the milk of this product is low, but breastfeeding women
should still suspend breastfeeding when taking the drug.
[Children's medication]
The safety and efficacy of this product in preterm infants and neonates
have not been determined, and the use of this product is not recommended
for premature infants and newborns under 1 month of age. For pediatric
patients over 1 month of age, see the recommended dosage under "Dosage".
[Medication for the elderly]
In a clinical trial of 920 patients treated with cefazolin, 313
participants (34%) were aged 65 years and older, and 138 participants
(15%) were aged 75 years and older. There was no overall difference in
the safety and efficacy of this product in these elderly subjects
compared to younger subjects. Other clinical reports have not shown
significant differences between older and younger patients, but the
possibility that a small number of older patients are more sensitive to
this product cannot be ruled out.
This product is excreted by the kidneys, so patients with renal
insufficiency may be at greater risk of toxic reactions. Elderly
patients usually have reduced kidney function, so the T1/2 of this
product is significantly longer than that of young people in the
elderly, and the dosage should be appropriately reduced or extended
according to the changes in kidney function.
[Drug Interactions]
1. This product is combined with gentamicin or amikacin to enhance the antibacterial effect in vitro.
2. The combination of cefazolin and warfarin increases the risk of
bleeding due to reduced synthesis of vitamin K-dependent coagulation
factors.
3. Cefazolin is combined with live typhoid vaccine, and the immune effect of the latter is reduced.
4. This product may increase nephrotoxicity when used with
anti-infective drugs (such as aminoglycosides, polymyxin E, polymyxin
B), iodine-containing contrast agents, organoplatinum compounds,
high-dose methotrexate, certain antiviral drugs (such as acyclovir,
sodium phoscarnate), cyclosporine, tacrolimus and diuretics (such as
furosemide), and it is recommended to monitor renal function.
5. When cefazolin is combined with probenecid, probenecid may reduce the
renal tubular secretion of cephalosporins, and probenecid can lead to
an increase in the blood concentration of this product and a prolonged
blood half-life.
6. Cefazolin contains methiontetrazezole side chains, and
alcohol-containing beverages or intravenous injection of
ethanol-containing drugs can cause alcohol-withdrawal sulfur-like
reactions (also known as disulfiram-like reactions) during medication.
[Drug overdose]
This product has no specific antagonists, and is mainly given
symptomatic treatment and a large amount of water and rehydration in
case of drug overdose.
[Pharmacology and Toxicology]
Pharmacological effects
Mechanism of action
Cefazolin is a fungicide that works by inhibiting the synthesis of bacterial cell walls.
Drug resistance
The main mechanisms of bacterial resistance to cephalosporins include
the presence of ultra-broad-spectrum β-lactamase (ESBL) and enzymatic
hydrolysis.
Antimicrobial profile
Cefazolin has antimicrobial activity against most strains of the following microorganisms in vitro and clinical infection:
Gram-positive bacteria
Staphylococcus aureus
Staphylococcus epidermidis
Streptococcus lactate
Streptococcus pneumoniae
Streptococcus pyogenes
Methicillin-resistant staphylococci are resistant to cefazolin.
Gram-negative bacteria
Escherichia coli
Proteus miraculous
Most indole-positive Proteus strains, Enterobacteriaceae, Morganella,
Providence resii, Serratia, and Pseudomonas are resistant to cefazolin.
Sensitivity test method
Where possible, clinical microbiology laboratories should regularly
report to physicians and provide the results of in vitro susceptibility
tests of antimicrobials used in their hospitals, which reflect the
susceptibility characteristics of hospital- and community-acquired
pathogens. These reports help doctors choose antimicrobials when
treating.
Dilution method
Dilution is a quantitative method for determining the MIC value of
antimicrobials. These MICs are used to assess bacterial sensitivity to
antimicrobials. MIC should be determined using standard test methods (if
feasible, broth and/or agar). The MIC values obtained should be
interpreted according to the criteria provided in Table 4.
Diffusion method
Paper diffusion is a quantitative method for measuring the diameter of
the inhibition zone and can also provide reproducible assessment of
bacterial sensitivity to antimicrobials. The size of the inhibition zone
can be used to evaluate the sensitivity of bacteria to antimicrobials.
Standard test methods should be used to determine the size of the
inhibition zone. This method tests microbial sensitivity to cefazolin by
using a paper piece impregnated with 30 μg cefazolin. Table 3 provides
the criteria for the paper diffusion method.
| Table 3. Sensitivity test criteria for cefazolin a | ||||||
| Pathogenic bacteria | Minimum inhibitory concentration (μg/mL). | Paper diameter (mm) b for diffusion method b | ||||
| S | I | R | S | I | R | |
| Enterobacteriaceae | ≤1 | 2 | ≥4 | - | - | - |
注: S: 敏感(Susceptible);I: 中介(Intermediate);R: 耐药(Resistant)
aThe judgment criterion is based on 1 g every 8 hours.
B cefazolin sheets should not be used to determine sensitivity to other cephalosporins.
Note :
Penicillin MIC ≤0.12 μg/mL for Streptococcus pyogenes and Streptococcus
agalactiacus, or a paper diffusion zone containing 10 μg penicillin ≥
24 mm in diameter, may be interpreted as sensitivity to cefazolin.
Note : Staphylococcal sensitivity to cefazolin can be inferred by testing for cefoxitin or oxacillin.
The report as "sensitive" means that if the antimicrobial reaches a
concentration that inhibits the growth of pathogens at the site of
infection, it is likely to inhibit pathogen growth. Reporting as
"mediated" means that the results are ambiguous and that the trial
should be repeated if the microorganism is not completely sensitive to
the alternative clinically viable drug. This means that the possible
clinical application is for use in body parts where the drug is
physiologically aggregated or in the case of high doses. It also
provides a buffer interval to prevent uncontrolled technical factors
from causing significant differences in judgment. Reporting "drug
resistance" means that antimicrobials cannot inhibit the growth of
pathogens at the site of infection, and other treatments should be
chosen.
Quality control
Standard sensitivity test methods enable the use of test controls,
quality control and guarantee the accuracy and precision of test
materials and reagents, as well as the individual techniques used to
conduct the test. Standard cefazolin powders should provide the MIC
value range in Table 4 below. The diffusion method uses 30 μg sheets of
paper and should meet the criteria in Table 4.
| Table 4. Acceptable quality control ranges for cefazolin | ||
| Quality control strains | Minimum inhibitory concentration (MIC) (μg/ml). | Diameter of the inhibition zone (mm). |
| Escherichia coli ATCC25922 | 1.0~4.0 | 21~27 |
| Staphylococcus aureus ATCC29213 | 0.25~1.0 | - |
| Staphylococcus aureus ATCC25923 | - | 29~35 |
Toxicology Research
Reproductive toxicity: No impairment of fertility or damage to the fetus due to cefazolin was
found in reproductive toxicity studies in rats, mice, and rabbits (at
doses up to 25 times the human dose).
[Pharmacokinetics]
Clinically, Cefazolin Sodium for Injection is used for intramuscular, intravenous or intravenous infusion.
Absorb
After intramuscular injection of 500mg of this product, the peak time
(tmax) of blood concentration is 1~2 hours, the peak blood concentration
(Cmax) reaches 38mg/L (32~42mg/L), the blood concentration can still be
measured at 7mg/L at 6 hours, and 3mg/L after 8 hours; After
intramuscular injection of 14.9 mg/kg, the Cmax reached at 2 hours was
52.2 mg/L. Intravenous infusion of 0.5g of this product within 20
minutes, the peak blood concentration (Cmax) is 118mg/L, and the
effective concentration is maintained for 8 hours; The same dose was
added to 100ml of glucose injection and intravenous infusion was given
within 30 minutes, and the Cmax could reach 143.6mg/L.
distribution
The distribution volume of cefazolin is 0.12L/kg, which is smaller than
other cephalosporins, and it is difficult for this product to penetrate
the blood-cerebrospinal fluid barrier, and the drug concentration cannot
be measured in the inflamed cerebrospinal fluid. Cefazolin can reach
higher concentrations in pleural effusion, ascites, pericardial fluid,
and bursal fluid. The average concentrations at 30 minutes, 60 minutes,
and 120 minutes after intravenous administration were 37mg/L, 15mg/L,
and 12mg/L, respectively. The average concentrations were 9 mg/L, 15
mg/L and 33 mg/L at 60 minutes, 120 minutes and 240 minutes after
intramuscular injection of 0.5 g, respectively. The concentration in
ascites was 90% of the blood concentration in the same period. The
concentration of the drug in the inflammatory exudate is basically equal
to the serum concentration; The concentration in bile is equal to or
slightly exceeds the plasma concentration in the same period, and after
the general therapeutic dose is given, the concentration of cefazolin in
bile is 17~31 mg/L, and the maintenance time is longer than that of
cefothiophene.
Protein binding
The protein binding rate of this product is 74%~86%.
Metabolism
This product is not metabolized in the body; The original drug is
filtered through the glomeruli and partially excreted in the urine
through the renal tubules.
Clear
The half-life of blood elimination (t1/2β) in normal healthy adults is 1.5~2 hours.
80%~90% of the administered dose can be excreted within 24 hours, and
the peak concentration of urine drug after intramuscular injection of
0.5g reaches 2400mg/L. Only a small amount (0.13%) of the drug is
excreted from the bile, but the concentration of the drug in the bile
remains high. Probenecid can increase the blood concentration by about
30% and prolong the effective blood concentration time.
Hemodialysis clears cefazolin slowly, and the blood concentration
decreases by 40%~50% after 6 hours of hemodialysis. Peritoneal dialysis
generally cannot remove this product.
Pharmacokinetics in special populations
children
For the distribution of cefazolin, after intravenous administration of
50mg/kg per day, the concentration in pus was 5.5~13.3mg/L and the
intraosseous concentration was 3.2~5.5mg/kg. The fetal blood
concentration is 70%~90% of the maternal blood concentration, and the
content in milk is low. The half-life of blood elimination (t1/2β) of
newborns within 1 week of birth is 4.5 ~ 5 hours.
Elderly
The half-life of blood elimination (t1/2β) in the elderly can be extended to 2.5 hours.
Patients with renal insufficiency
In patients with renal impairment, the serum half-life is prolonged, and
the duration of serum concentrations depends on the degree of renal
impairment. For example, the half-life of blood elimination (T1/2β) in
patients with renal failure can be prolonged, and the clearance rate of
endogenous creatinine is 12~17ml/min and less than 5ml/min is 12 hours
and 57 hours, respectively.
[Storage]
Keep away from light, airtight, and store no more than 25°C.
[Packaging]
Medium borosilicate glass injection bottles, sterile powders for
injection, tetrafluoroethylene copolymer film co-cloride butyl rubber
stoppers and antibiotic bottles are packaged with aluminum-plastic
combination caps, (1) 1 bottle per box, (2) 10 bottles per box.
[Validity period]
30 months
[Implementation standards]
The National Medical Products Administration has YBH08912021 standards
[Approval number]
Sinopharm standard word H20204005 (1.0g).
[Drug marketing authorization holder]
Company name: Guangdong Jincheng Jinsu Pharmaceutical Co., Ltd
Registered address: No. 10, Shennong Road, Torch Development Zone, Zhongshan City, Guangdong Province
[Manufacturer]
Company name: Guangdong Jincheng Jinsu Pharmaceutical Co., Ltd
Production address: No. 10 Shennong Road, Torch Development Zone, Zhongshan City, Guangdong Province
Postal code: 528437
Service hotline: 400-9988-970
Telephone number: (0760) 22830525 (switchboard).
Fax number: (0760) 22578279
Website: http://www.gdjcjs.com