 CN
CN
Cefoperazone Sodium and Sulbactam Sodium for Injection
Instructions for Cefoperazone Sodium and Sulbactam Sodium for Injection
Please read the instructions carefully and use under the guidance of a physician or pharmacist
[Name of the drug]
Generic name: Cefoperazone Sodium and Sulbactam Sodium for Injection
Product name: Cefoperazone Sodium and Sulbactam Sodium for Injection
Hanyu Pinyin: Zhusheyong Toubaopaitongna Shubatanna 【 Ingredients 】
This product is a compound preparation, the active ingredients are
cefoperazone sodium and sulbactam sodium (cefoperazone and sulbactam are
1:1), and no excipients are included.
Cefoperazone sodium
Chemical Name: (6 R R,7 R )-3-[[(1-methyl-1H-tetrazole-5-yl H)sulfur]methyl]-7-[( R ).
)-2-(4-ethyl-2,3-dioxo-1-piperazinecarbonylamino)-2-p-hydroxyphenyl-acetylamino]-8-oxo-5-thio-1-azabicyclic
[4.2.0]oct-2-en-2-carbamate sodium salt.
Chemical structural formula:
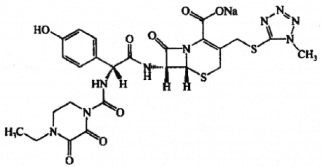
Molecular formula:C 25 H 26 N 9 NaO 8 S 2
Molecular weight: 667.65
Sulbactam sodium
Chemical Name: ( S2S,5R R)-3,3-dimethyl-7-oxo-4-thio-za-1-azabicyclic [3.2.0]Sodium heptane-2-carboxylate-4,4-dioxide.
Chemical structural formula:
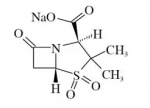
Molecular formula: C 8 H 10 NNaO 5 S
Molecular Weight: 255.22
According to the amount indicated on the label, this product contains
32mg of sodium per bottle of 0.5g size, 64mg of sodium per bottle of
1.0g size, 96mg of sodium per bottle of 1.5g size, and 128mg of sodium
per bottle of 2.0g size.
[Characteristics]
This product is a white or white-like powder.
[Indications]
Medication alone
Cefoperazone/sulbactam is indicated for the treatment of the following infections caused by sensitive bacteria:
1) Upper and lower respiratory tract infections;
2) Upper and lower urinary tract infections;
3) peritonitis, cholecystitis, cholangitis and other intra-abdominal infections;
4) sepsis;
5) meningitis;
6) skin and soft tissue infections;
7) Bone and joint infections;
8) Pelvic inflammatory disease, endometritis, gonorrhea, and other genital tract infections.
Combination medication
Because of its broad-spectrum antibacterial activity,
cefoperazone/sulbactam can treat most infections on its own, but
cefoperazone/sulbactam is sometimes used in combination with other
antibiotics. When this product is combined with aminoglycoside
antibiotics (participate in the aminoglycoside antibiotic part of [drug
interaction] compatibility contraindication), the patient's renal
function should be monitored during treatment (participate in the
medication part of patients with renal dysfunction in [Dosage]).
[Specifications]
1.5g(C 25 H 27 N 9 O 8 S 2 0.75g 与 C 8 H 11 NO 5 S 0.75g)
[Usage and dosage]
Adult medication
The recommended daily dose of cefoperazone/sulbactam for adults is as follows:
| proportion | Cefoperazone / sulbactam ( g ). | Cefoperazone ( g ). | Sulbactam ( g ). |
| 1 : 1 | 2.0~4.0 | 1.0~2.0 | 1.0~2.0 |
The above doses are
administered in equal doses every 12 hours. The daily dose of
cefoperazone/sulbactam can be increased to 8g (1:1
cefoperazone/sulbactam, i.e., 4g cefoperazone) when treating severe or
refractory infections. When the condition requires,
Patients receiving 1:1 cefoperazone/sulbactam may be additionally
increased in cefoperazone separately at equal doses administered every
12 hours. The maximum recommended daily dose of sulbactam is 4g.
Medication for patients with hepatic dysfunction : See [Precautions].
Medication for patients with renal dysfunction
Patients with significantly reduced renal function (creatinine clearance
<30 ml/min) with decreased clearance of sulbactam should adjust the
regimen of cefoperazone/sulbactam. The maximum daily dose of sulbactam
for patients with creatinine clearance of 15~30ml/min is 2g in equal
doses every 12 hours. The maximum daily dose of sulbactam in patients
with creatinine clearance < 15 ml/min is 1 g in equal doses every 12
hours. In case of severe infection, the dose of cefoperazone can be
increased separately if necessary.
In hemodialysis patients, the pharmacokinetic properties of sulbactam
are significantly altered. The serum half-life of cefoperazone is
slightly shortened in hemodialysis patients. Therefore, it should be
given after the end of hemodialysis.
Intravenous administration
1) When using intermittent intravenous infusion, each bottle of
cefoperazone/sulbactam should be dissolved with an appropriate amount of
5% glucose solution or 0.9% injection with sodium chloride solution or
sterile water for injection (refer to [Dosage] for the dissolution part
of this product), and then diluted to 20ml with the same solution
mentioned above, and the intravenous infusion time should be at least
15~60 minutes.
Although Sodium Lactate Ringer Injection can be used as a solvent for
cefoperazone/sulbactam IV injection, it cannot be used in the initial
dissolution process of this product (see [Drug Interactions] Compatibility Contraindications Sodium Ringer Lactate Injection and [Dosage] Use 用/ Operation Instructions ). Sodium lactate Ringer injection part).
2) When using intravenous bolus, each bottle of cefoperazone/sulbactam
should be dissolved in the above way, and the intravenous bolus time
should be at least more than 3 minutes.
Intramuscular injection
Although 2% lidocaine hydrochloride injection can be used as a solvent
for cefoperazone/sulbactam intramuscular injection, it cannot be used in
the initial dissolution process of this product (see [Drug
Interactions] Compatibility Contraindications for Lidocaine and [Dosage] Instructions for Use / Operation of Lidocaine).
Instructions for use / operation
1) Dissolution of this product
This product can be dissolved per 1.0g of cefoperazone/sulbactam according to the table below.
| Total dose ( g ). | Equivalent to the dose (g) of cefoperazone + sulbactam (g) | Volume of dilution ( ml ). | Highest final concentration ( mg/ml ). |
| 1.0 | 0.5+0.5 | 3.4 | 125+125 |
Cefoperazone/sulbactam can be
combined with water for injection, 5% glucose injection, normal saline,
5% glucose and 0.225% sodium chloride injection within the concentration
range of 10~250mg/ml and 5~125mg/ml for cefoperazone and sulbactam,
respectively
5% glucose and 0.9% sodium chloride injection are compatible.
2) Sodium lactate Ringer injection
Cefoperazone/sulbactam should be dissolved with sterile water for injection (see [Drug Interactions] Compatibility Contraindications Sodium Lactate Ringer Injection). A two-step dilution method was used:
first dissolved in sterile water for injection (as shown in the table
above), then diluted with sodium Ringer Lactate Injection to a solution
of 5mg/ml of sulbactam (diluted with 2ml of primary solution to 50ml of
Sodium Lactate Ringer Injection or 4ml of initial solution diluted to
100ml Sodium Lactate Ringer Injection).
3) Lidocaine
Cefoperazone/sulbactam should be dissolved in sterile water for injection (see [Drug Interactions] Compatibility Contraindications to Lidocaine). A two-step dilution method should be used: first
dissolved in sterile water for injection (as shown in the table above),
and then diluted with 2% lidocaine solution to achieve concentrations of
125mg/ml and 125mg/ml of cefoperazone and sulbactam in about 0.5%
lidocaine hydrochloride solution, respectively.
[Adverse reaction]
Adverse reactions and laboratory abnormalities were observed in 1023
(7.99%) of a total of 12,808 patients (at the time of completion of
review) after the development study and approval of the study. The main
adverse reaction was diarrhea
(0.75%), rash (0.45%), fever (0.21%), etc. The main laboratory
abnormalities were elevated ALT (3.41%), elevated AST (3.18%), and
elevated ALP (1.05%).
Clinically significant adverse effects (incidence unknown due to spontaneously reported causes.) )
1) Shock, anaphylactic shock / anaphylaxis (dyspnea, etc .):
In the event of shock, anaphylactic shock/anaphylaxis, etc., the patient
should be closely monitored. If any abnormal results are observed, the
administration should be discontinued immediately and appropriate
treatment measures should be taken.
2 ) Acute renal failure:
Because severe kidney impairment such as acute kidney failure can occur,
regular laboratory tests are necessary. If any abnormal results are
observed, appropriate therapeutic measures should be taken, such as
interrupting dosing.
3 ) Pseudomembranous colitis:
Severe colitis such as pseudomembranous colitis with bloody stools may
occur. When abdominal pain or frequent diarrhea occurs, appropriate
treatment measures should be taken, such as interrupting the
administration.
4 ) Interstitial pneumonia, PIE syndrome:
Interstitial pneumonia with fever, cough, dyspnea, abnormal x-rays or
eosinophils, and pulmonary infiltrates with eosinophilic syndrome may
occur. If such symptoms are observed, the drug should be stopped
immediately and appropriate treatment should be taken, such as
adrenocorticosteroids.
5 ) Mucosa-skin-ocular -皮肤- syndrome ( Stevens Johnson syndrome) and toxic epidermal necrolysis (Lyell's syndrome):
Mucosa-skin-eye syndrome (Stevens Johnson syndrome) and toxic epidermal necrolysis may occur
(Lyell syndrome). If such symptoms are observed, the administration
should be interrupted immediately and appropriate treatment measures
should be taken.
6 ) Blood dyshydration:
Severe blood dyshydra such as hemolytic anemia, pancytopenia,
granulocytopenia (including agranulocytosis), thrombocytopenia, etc. may
occur, and it is necessary to take measures such as careful observation
through regular laboratory tests. If any abnormal results are observed,
appropriate treatment should be taken, such as interrupting dosing.
7 ) Fulminant hepatitis:
Because fulminant hepatitis can occur, it is necessary to take measures
such as careful observation through regular laboratory tests. If any
abnormal results are observed, appropriate therapeutic measures should
be taken, such as interrupting dosing.
Adverse events are typically collected from reports during clinical
trials and after the product is launched. Many events can be caused by
factors other than medication, such as latent disease. Since it is not
possible to determine a specific causal relationship in most cases (and
even many adverse events are not adverse drug reactions), we report all
adverse events collected here, even when it is not possible to determine
whether it is caused by cefoperazone/sulbactam.
Cefoperazone/sulbactam is generally well tolerated, with most adverse
effects being mild or moderate and tolerable without affecting continued
treatment. The following adverse effects have been observed from
clinical trials (comparative and non-comparative studies) and
post-marketing experience.
All adverse reactions in the package inserts are listed according to the
MedDRA system classification and are ranked by clinical importance.
Adverse reaction table
| Systematic organization classification | Very common ≥ 1/10 | Common ≥ 1/100 to<1/10 |
Rare ≥1/1000 to<1/100 |
The frequency is unknown (None according to available data Legal estimate). |
| blood and lymphatic system The system is abnormal |
Neutropenia† leukocytes Reduce † and direct Combs test positive Sexual reaction †, hemoglobin drops † Decreased hematocrit † platelets Reduce † |
Coagulation disorders*, eosinophilia There are many † |
Platelets | Vitamin K deficiency (low Prothrombinemia*, bleeding tendency, etc.), anemia |
| Abnormal immune system | anaphylactic shock*§, allergic Reaction*§, anaphylaxis§ (including shock*), hypersensitivity should *§ |
|||
| Neurological abnormalities | Headache | Convulsions | ||
| Vascular abnormalities | Bleeding*§, vasculitis*, hypoheemia Press* |
|||
| Gastrointestinal abnormalities | diarrhea, nausea, Vomiting |
Loose manure | Pseudomembranous enteritis*, stomatitis, candidiasis | |
| Abnormalities in the liver and bile ducts | Alanine aminotransferase is elevated† aspartate aminotransferase is elevated† and blood alkaline phosphatase is elevated, † | Bilirubin is elevated † | Jaundice* | |
| Skin and subcutaneous groups Weaving is abnormal |
Itching, hives Measles, pesticides Rash |
Toxic epidermal necrolysis |
||
| kidneys and urinary system The system is abnormal |
Hematuria* | |||
| General abnormalities and administration sites | Veins at the injection site inflammation, injection site |
B vitamin deficiency (glossitis, anorexia, god | ||
| pain, fever, Chills |
Menstritis, etc.). |
*Post-marketing adverse reactions.
† all available laboratory values, including those with abnormal
baseline, are included in the calculation of the frequency of abnormal
laboratory adverse reactions. This conservative approach is used because
the raw data do not distinguish between patients with baseline
abnormalities with significant laboratory changes in treatment and
patients with baseline abnormalities without significant laboratory
changes. For leukocytes, neutrophils, platelets, hemoglobin, and
hematocrit, studies only reported abnormalities and did not distinguish
between elevated or decreased values.
§ There are reports of fatal incidents.
[Contraindication]
It is contraindicated in those who are known to be allergic to
penicillins, sulbactam, cefoperazone and other cephalosporin antibiotics
or have a history of shock to the ingredients of this product.
Patients with a history of hypersensitivity to the ingredients of this
product or cephalosporin drugs are generally prohibited from using
cefoperazone sodium for injection sulbactam sodium, and if it is really
necessary to use cefoperazone sodium for injection sulbactam sodium, it
should be administered with caution.
[Precautions]
Warning: Severe bleeding, including fatality, associated with
cefoperazone sodium for injection sulbactam has been reported. Bleeding,
thrombocytopenia, and signs of coagulation disorders should be
monitored. If there is unexplained persistent bleeding, the drug should
be discontinued immediately.
A small number of patients develop vitamin K deficiency leading to
coagulation disorders after treatment with this product, and the
mechanism is likely related to the inhibition of the gut flora that
synthesizes the vitamin, including malnutrition, malabsorption (eg,
patients with pulmonary cystic fibrosis), patients with alcohol
poisoning, and long-term intravenous infusion of highly nutritious
preparations. Hypothrombinemia (with or without bleeding) is reported.
Vitamin K deficiency causes bleeding tendencies. Prothrombin time should
be monitored in these patients and in patients treated with
anticoagulants, and vitamin K should be supplemented if needed.
Independent risk factors for bleeding may include an injury or condition
that increases the risk of clinically significant bleeding, such as a
recent cerebral infarction (ischemic or hemorrhagic); Active peptic
ulcer with recent bleeding; Patients with impaired spontaneous or
acquired hemostatic balance; Liver disease with coagulation disorders
and clinically relevant bleeding risk; Systemic concomitant use of
medications known to affect hemostasis.
1. Hypersensitivity
βSevere,
occasionally fatal hypersensitivity (anaphylactic) reactions, including
cefoperazone/sulbactam, have been reported in patients treated with
β-lactam or cephalosporin antibiotics. These reactions are more likely
to occur in patients with a history of hypersensitivity to multiple
allergens. In the event of an allergic reaction, the drug should be
stopped immediately and appropriate treatment should be given.
For patients with a tendency to cause allergic reactions such as bronchial asthma, rash, hives, etc. or the patient's parents
Parents, brothers, or sisters, should use cefoperazone sodium for injection with caution.
Patients with severe allergic reactions should be given emergency
treatment with epinephrine immediately, and if necessary, oxygen,
intravenous kinesis, and unobstructed airway including endotracheal
intubation should be used.
Serious epidemical, lethal cutaneous adverse reactions, such as toxic
epidermal necrolysis (TEN), Stevens-Johnson syndrome (SJS), and
exfoliative dermatitis, have been reported in patients treated with
cefoperazone/sulbactam. In the event of a severe skin reaction, the drug
should be discontinued immediately and appropriate treatment should be
given.
Because there is no definitive way to predict the occurrence of shock or
anaphylactoid shock associated with this type of drug, the following
measures must be taken:
1) Before treatment, the patient's relevant situation should be
understood in detail, so as to find out the patient's drug allergy
history. In particular, it is necessary to confirm whether the patient
has a history of antibiotic allergy.
2) Prior preparation for shock first aid should be carried out before treatment.
3) Patients should be kept quiet and closely monitored during the
administration of this drug. In particular, patients should be closely
monitored for a period of time after administration of this drug.
2. Medication for patients with liver dysfunction
Cefoperazone is mainly excreted through bile. When patients have liver
disease and/or biliary obstruction, the serum half-life of cefoperazone
is usually prolonged and the amount of drug excreted in the urine
increases. Even if the patient has severe liver dysfunction,
cefoperazone can still reach therapeutic concentrations in bile and its
half-life is only 2~4 times longer.
If you encounter severe biliary obstruction, severe liver disease, or renal dysfunction, you may need to adjust the dosage.
Patients with hepatic dysfunction and renal impairment should monitor
the serum concentration of cefoperazone and adjust the dose as needed.
The daily dose of cefoperazone should not be exceeded in these patients
if serum concentrations of this product are not closely monitored
2g。
3. General Notes
Severe bleeding cases have been reported with cefoperazone/sulbactam,
including fatal. As with other antibiotics, a small number of patients
develop vitamin K deficiency leading to coagulation disorders after
treatment with cefoperazone/sulbactam, and the mechanism is likely
related to the inhibition of the gut microbiota that synthesizes the
vitamin, including malnutrition, malabsorption (eg, in patients with
pulmonary cystic fibrosis), and long-term intravenous infusion of highly
nutritious preparations. Vitamin K deficiency causes bleeding
tendencies.
Prothrombin time should be monitored in these patients and in patients
treated with anticoagulants, and vitamin K should be supplemented if
needed. If there is unexplained persistent bleeding, the drug should be
discontinued immediately.
As with other antibiotics, long-term use of cefoperazone/sulbactam can
cause an overgrowth of insensitive bacteria. Therefore, in
During treatment, the patient's condition changes should be carefully
observed. As with other systemic antibiotics, it is recommended that the
patient be regularly examined for dysfunction of various systems and
organs, including the kidneys, liver, and blood system, during a longer
course of treatment. This is especially important for newborns,
especially premature babies and other babies.
4. Clostridium difficile associated diarrhea C (DAD) has been reported
in almost all antimicrobial applications, including cefoperazone
sodium/sulbactam sodium, which can manifest in severity from mild
diarrhea to fatal enteritis. Antimicrobial therapy can cause changes in
the normal flora of the colon, leading to the overgrowth of Clostridium
difficile.
Toxin A and toxin B produced by Clostridium difficile are associated
with the pathogenesis of CDAD. The highly toxin-producing Clostridium
difficile leads to increased morbidity and mortality, and these
infections may not be refractory to antimicrobial therapy and may
require colon resection. The possibility of CDAD must be considered in
all patients with diarrhea after antibiotic use. Because CDAD has been
reported more than 2 months after antimicrobial therapy, a careful
history should be asked.
5. Impact on the ability to drive and operate the machine
Experience with cefoperadone/sulbactam clinical use shows that it does
not reduce the patient's ability to drive and operate the machine.
[Medication for pregnant and lactating women]
Medication during pregnancy
Reproductive studies have been conducted in rats, using doses up to 10
times the human dose, and no fertility has been found to be impaired,
nor has any teratogenic effect of the drug been found. Both sulbactam
and cefoperazone can cross the placental barrier, but adequate and
well-controlled trials have not been conducted in pregnant women. Since
the results of animal reproduction studies do not always predict the
human condition, pregnant women should only use this product if the
doctor deems it necessary.
Lactation medication
Only small amounts of sulbactam and cefoperazone are secreted into the
body's breast milk. Although only small amounts of sulbactam and
cefoperazone can enter breast milk, breastfeeding women should use this
product with caution.
[Children's medication]
The recommended daily dose of cefoperazone/sulbactam for children is as follows:
| proportion | Cefoperazone / sulbactam ( mg/kg ). | Cefoperazone ( mg/kg ). | Sulbactam ( mg/kg ). |
| 1 : 1 | 40~80 | 20~40 | 20~40 |
The above doses are divided into equal doses and injected every 6 to 12 hours.
The above dose can be increased to 160mg/kg per day in a 1:1 ratio when treating severe infections or refractory infections
Administer in equal doses 2~4 times a day (see [Children's Medication] Infant Medication and [Pharmacology and Toxicology] Toxicology Studies).
Neonatal medication
Newborns in the first week of life should be given every 12 hours. The
maximum daily dose of sulbactam in children should not exceed 80 mg/kg
per day (see Pediatric Medications for Infants and Pharmacology and Toxicology). Toxicological research
Infant medication
Cefoperazone/sulbactam has been used effectively in the treatment of
infections in infants. Extensive research has not been done in preterm
infants and neonates, so physicians should weigh the pros and cons
before using cefoperadone/sulbactam in preterm and neonatal infants.
Cefoperazone does not replace bilirubin from plasma protein binding sites.
[Medication for the elderly]
See [Clinical Pharmacology] Pharmacokinetics for Elderly Patients.
[Drug Interactions]
Interaction with alcohol
Alcohol consumption during cefoperazone and within 5 days of
discontinuation has been reported to cause characteristic reactions such
as flushing, sweating, headache, and tachycardia, and similar reactions
have been reported with some other cephalosporins. Therefore, patients
should be careful when using cefoperazone/sulbactam when drinking
alcoholic beverages at the same time. When patients require enteral or
parenteral nutrition, they should avoid giving liquids containing
alcohol.
Drug interactions in laboratory tests
False positives can occur when urine glucose is checked with Bennedict solution or Fehling reagent.
Compatibility taboos
1) Aminoglycoside antibiotics
Since there are physical compatibility contraindications between
cefoperazone/sulbactam and aminoglycoside antibiotics, the two solutions
cannot be mixed directly. If cefoperazone/sulbactam is required in
combination with aminoglycoside antibiotics (see [Indications] Combination Administration), sequential intermittent intravenous infusion may be
used, but a different IV line must be used, or the previously used IV
line must be fully flushed with an appropriate dilution during the
interfusion period. In addition, it is recommended that the interval
between cefoperazone/sulbactam and aminoglycoside antibiotics be as long
as possible during the whole day.
2) Sodium lactate Ringer injection
Since this product has compatibility contraindications after mixing with
Sodium Lactate Ringer Injection, the use of this solution should be
avoided when it is initially dissolved. In the two-step dilution method,
the initial dissolution is carried out with water for injection, and
then further diluted with sodium Ringer lactate injection to obtain a
mixture that can be compatible with each other (see [Dosage] Instructions for Use / Operation 说明 Sodium Ringer Injection section).
3) Lidocaine
Since this product has compatibility contraindications when mixed with
2% lidocaine hydrochloride injection, the use of this solution should be
avoided when it is initially dissolved. In the two-step dilution
method, the initial dissolution is carried out with water for injection,
and then further diluted with 2% lidocaine hydrochloride injection to
obtain a mixture that can be compatible with each other (see the
Lidocaine section of the [Dosage] Use / Operation Instructions ).
4) When this product is used at the same time as drugs that can produce
hypothrombinemia, thrombocytopenia or gastrointestinal bleeding, the
effect of these drugs on coagulation function and increased risk of
bleeding should be considered.
[Drug overdose]
There is little information on acute human poisoning of cefoperazone
sodium and sulbactam sodium. The expected clinical manifestations of
overdose of this product are mainly those that have been reported to be
magnified. High concentrations of ββ-lactam
antibiotics in cerebrospinal fluid can cause adverse reactions of the
central nervous system, such as convulsions. Since both cefoperazone and
sulbactam are removed from the blood circulation by hemodialysis,
hemodialysis treatment can increase the excretion of this product from
the body in the event of an overdose in patients with renal impairment.
[Clinical Pharmacology]
Pharmacokinetics
After cefoperazone/sulbactam injection, about 84% of sulbactam and 25%
of cefoperazone are excreted by the kidneys, and most of the remaining
cefoperazone is excreted through bile. After cefoperazone/sulbactam
injection, the average half-life is about 1 hour for sulbactam and 1.7
hours for cefoperazone. Blood concentration is proportional to the dose
administered. The values are consistent with the published values used
separately for the two.
After 5 minutes of intravenous administration of 2g
cefoperazone/sulbactam (1g cefoperazone and 1g sulbactam), the mean peak
blood concentrations of cefoperazone and sulbactam were 236.8μg/ml and
130.2μg/ml, respectively, suggesting that the distribution volume of
sulbactam (Vd =18.0~
27.6L) was greater than the volume of distribution of cefoperazone (Vd =10.2~11.3L).
After intramuscular administration of 1.5g of cefoperadone/sulbactam (1g
cefoperazone, 0.5g sulbactam), serum concentrations of sulbactam and
cefoperazone peaked at 15 minutes to 2 hours, and the mean serum peak
concentrations of cefoperazone and sulbactam were respectively
64.2μg/ml 和 19.0μg/ml。
Both cefoperazone and sulbactam are well distributed to various tissues
and body fluids, including bile, gallbladder, skin, appendix, fallopian
tubes, ovaries, uterus, and other tissues and body fluids.
There is no evidence of pharmacokinetic interactions between the two
components after injection of the cefoperazone/sulbactam combination
formulation.
It has been reported that there is no significant change in the
pharmacokinetic parameters of the two components after multiple doses of
cefoperadone/sulbactam, and no drug accumulation is observed when
injected every 8~12 hours.
Medication for patients with liver dysfunction
See the [Notes] section.
Medication for patients with renal dysfunction
After cefoperazone/sulbactam injection in patients with varying degrees
of renal dysfunction, the total drug clearance of sulbactam was closely
related to the estimated creatinine clearance. In patients with renal
failure, the half-life of sulbactam was significantly extended (on
average 6.9 hours and 9.7 hours in both studies). In hemodialysis
patients, the half-life, total drug clearance and apparent volume of
distribution of sulbactam were significantly altered. No significant
differences in the pharmacokinetic parameters of cefoperazone were
observed in patients with renal failure.
Medication for elderly patients
Pharmacokinetic parameters of cefoperazone/sulbactam were studied in
older adults with renal dysfunction and impaired hepatic function, and
both sulbactam and cefoperazone showed prolonged half-lives, decreased
drug clearance, and increased apparent volume of distribution compared
to normal healthy subjects. The pharmacokinetic parameters of sulbactam
are highly correlated with the degree of impairment of renal function,
while the pharmacokinetic parameters of cefoperadone are closely related
to the degree of impairment of liver function.
Medication for children
Studies in pediatric patients showed no significant change in the
pharmacokinetic parameters of the cefoperazone/sulbactam components
compared to adult data. The half-life of sulbactam in children ranges
from 0.91 to 1.42 hours and for cefoperazone from 1.44 to 1.88 hours.
[Pharmacology and Toxicology]
Pharmacological effects
The antibacterial component of cefoperazone/sulbactam is cefoperazone,
which is a third-generation cephalosporin that achieves bactericidal
effect by inhibiting the biosynthesis of cell wall mucopeptides of
sensitive bacteria during the bacterial reproduction period. Sulbactam
does not have any effective antibacterial activity against other
bacteria except Neisseriaceae and Acinetobacter. However, biochemical
studies with bacteria have shown that sulbactam has irreversible
inhibitory effects on most important β-lactamases produced by
antibiotic-resistant strains of β-lactam classes.
The study of drug-resistant bacteria in whole cells confirmed that
sulbactam can prevent the destruction of penicillin and cephalosporin
antibiotics by drug-resistant bacteria, and that sulbactam has obvious
synergistic effect with penicillin and cephalosporin antibiotics.
Because sulbactam can bind to certain penicillin-binding proteins,
sensitive strains are generally more sensitive to cefoperazone/sulbactam
than to cefoperazone alone.
The cefoperazone/sulbactam combination has antimicrobial activity
against all cefoperazone-sensitive bacteria. In addition, it showed
synergistic antibacterial effects on a variety of bacteria, especially
the following bacteria (the minimum inhibitory concentration (MIC) value
of the cefoperazone/sulbactam combination was reduced by up to 4 times
compared with the single component).
Haemophilus influenzae
Bacteroidetes
Staphylococcus spp
Acinetobacter calcium acetate Enterobacteriaceae aerogeniensis
E. coli
Proteus miraculous
Pneumoniae Klein
Morganella Morse
Citrate bacteria fraudi Enterobacteriaceae claude
Heteromorphic citric acid bacillus
In vitro tests, cefoperadone/sulbactam has antimicrobial activity against many clinically important pathogens:
Gram-positive bacteria:
Staphylococcus aureus, a strain that produces and does not produce penicillinase Staphylococcus epidermidis
Streptococcus pneumoniae (formerly known as pneumococcus).
Streptococcus pyogenes (group A) - Streptococcus hemolyticus).
Streptococcus agalactiac (group B 阝) Most strains of Streptococcus agaemolyticus
Many strains of Enterococcus faecalis gram-negative bacteria:
E. coli
Craig albaifungus
Enterobacteriaceae
Citrate acid bacteria
Haemophilus influenzae Proteus mirabacter common Proteus commonis
Morganella moseii (formerly known as Proteus mogi
Providence reiferi (formerly known as Proteus reiferi).
Providence fungi
Serratia spp. (including Serratia marcescens) Salmonella and Shigella spp
Pseudomonas aeruginosa and certain other pseudomonas belong to Acinetobacter acetate
Gonococcus
Meningococcus pertussis bacillus
enterocolitis Yersinia anaerobic bacteria:
Gram-negative bacilli (including Bacteroidetes fragilis, other Bacteroidetes, and Fusobacterium).
Gram-positive and gram-negative cocci (including Pyrococcus, Pyrococcus,
and Veronella spp.) Gram-positive bacilli (including Clostridium,
Eobacterium, and Lactobacillus spp
The established sensitivity ranges for cefoperazone/sulbactam are shown below:
Minimum inhibitory concentration ( MIC ), ( μg/ml , in terms of cefoperazone concentration).
| Sensitive | ≤16 |
| Moderately sensitive | 17~63 |
| Drug resistance | ≥64 |
Diameter of the sensitive paper inhibition zone , ( mm , Kirby-Bauer method).
| Sensitive | ≥21 |
| Moderately sensitive | 16~20 |
| Drug resistance | ≤15 |
Stepwise dilution of
cefoperadone/sulbactam at a ratio of 1:1 or 2:1 by broth dilution or
agar dilution method to obtain its lowest bacteriostatic concentration
(MIC). Susceptibility paper containing 75 μg cefoperazone and 30 μg
sulbactam is recommended. If the sensitivity test reports "sensitive",
indicating that cefoperazone/sulbactam may be effective in treating
infecting pathogens; If "drug resistance" is reported, it indicates that
cefoperazone/sulbactam may not be effective in treating the infected
pathogen; A report of "moderate sensitivity" indicates that the pathogen
may be sensitive to cefoperazone/sulbactam if given at a higher dose or
when the infection is confined to tissues or body fluids with high
concentrations of this product.
The following recommendations are the quality control criteria for the 75 μg/30 μg cefoperazone/sulbactam susceptibility test:
| Control strains | Diameter of the inhibition zone (mm). |
| Acinetobacter genus, ATCC43498 | 26~32 |
| Pseudomonas aeruginosa, ATCC27853 | 22~28 |
| Escherichia coli, ATCC25922 | 27~33 |
| Staphylococcus aureus, ATCC25923 | 23~30 |
Toxicology Research
At present, there are no genotoxicity, reproductive toxicity (except for
subcutaneous administration, see cefoperazone part) and carcinogenicity
research data of this compound preparation, and the toxicological
studies of each single drug can refer to the following relevant data.
Cefoperazone
Genotoxicity: In vivo and in vitro genotoxicity studies have not found
that this product has mutagenic effects: the results of chromosomal
aberration test in human lymphocytes are negative, but when the whole
blood cell culture of this product is carried out, chromosomal breaks
are found to increase.
Reproductive toxicity: Daily subcutaneous injection of cefoperazone
1000mg/kg (approximately 16 times the average adult dose) can lead to
reduced testicular weight, inhibited spermatogenesis, decreased germ
cell number, and intracytoplasmic vacuole formation in rats. In the
range of 100~1000mg/kg per day, the severity of the damage is related to
the dose. Low doses can cause a slight reduction in sperm cells, which
is not observed in adult rats. This histological damage is reversible in
all dose groups except the highest dose. Nevertheless, these trials did
not evaluate later reproductive function in rats. The relationship
between the above findings and the human body has not been established.
Subcutaneous injection of cefoperadone/sulbactam in newborn rats, in a
ratio of 1:1 (daily dose of 300mg/kg+300mg/kg) after 1 month of
medication, can lead to a decrease in testicular weight in rats and the
appearance of immature tubules, due to the large individual differences
in the maturation of the testes of young rats, and immature testicles
were also found in the control group, so it is uncertain whether the
above phenomena are related to drugs. The above was not observed when
puppies were given more than 10 times the average adult dose of
cefoperazone/sulbactam.
Both sulbactam and cefoperazone can cross the placental barrier, but
have not been fully and rigorously tested in pregnant women. Since the
results of animal reproduction studies do not always predict the human
condition, pregnant women should only use this product if the doctor
deems it necessary. Lactation medication: Only a small amount of
sulbactam and cefoperazone can be secreted into the body's breast milk.
Although only a small amount of sulbactam and cefoperazone can enter
breast milk, breastfeeding women should still use it with caution.
Carcinogenicity: There are no studies on the potential carcinogenicity of this product for long-term use.
Shubactam
Genotoxicity: No studies have been reported.
Reproductive toxicity: No fertility damage and fetal toxicity were found
when administered to mice, rats, and rabbits at doses up to 10 times
the human dose. However, there is no sufficient and rigorous data on
pregnant women, and the relevance of animal studies to humans is
unclear.
Carcinogenicity: not reported in studies.
[Storage]
Keep away from light, airtight, and store no more than 25°C.
[Packaging]
Medium borosilicate glass molded injection bottles, aseptic powders for
injection, coated tetrafluoroethylene copolymer film for injection,
butyl chloride rubber stoppers and aluminum-plastic combination caps for
antibiotic bottles. 1 bottle/box, 10 bottles/box.
[Validity period]
18 months.
[ Implementation standards]
The National Medical Products Administration YBH03762023 standards
[ Approval number ]
1.5g(C 25 H 27 N 9 O 8 S 2 0.75g 与 C 8 H 11 NO 5 S 0.75g):国药准字 H20066402
[ Marketing authorization holder ]
Name: Guangdong Jincheng Jinsu Pharmaceutical Co., Ltd
Registered address: No. 10, Shennong Road, Torch Development Zone, Zhongshan City, Guangdong Province
【Manufacturer】 Company name: Guangdong Jincheng Jinsu Pharmaceutical Co., Ltd
Guangdong Jincheng Jinsu Pharmaceutical Co.,Ltd.
Production address: No. 10 Shennong Road, Torch Development Zone, Zhongshan City, Guangdong Province
Postal code: 528437
Service hotline: 400-9988-970
Telephone number: (0760) 22830525 (switchboard).
Fax number: (0760) 22578279
Website: http://www.gdjcjs.com